Pleasecitethisarticleinpressas:FráterM,etal.Fatiguebehaviorofendodonticallytreatedpremolarsrestoredwithdifferentfiber-reinforced designs.DentMater(2020),https://doi.org/10.1016/j.dental.2020.11.026
ARTICLE IN PRESS
DENTAL-3689; No.ofPages12
dental materials xxx (2020)xxx–xxx
Availableonlineatwww.sciencedirect.com
ScienceDirect
j ou rn a l h o m epa ge :w w w . i n t l . e l s e v i e r h e a l t h . c o m / j o u r n a l s / d e m a
Fatigue behavior of endodontically treated
premolars restored with different fiber-reinforced designs
Márk Fráter
a, Tekla Sáry
a, Blanka Jókai
a, Gábor Braunitzer
b,
Eija Säilynoja
c,d, Pekka K. Vallittu
c,e, Lippo Lassila
c, Sufyan Garoushi
c,∗aDepartmentofOperativeandEstheticDentistry,FacultyofDentistry,UniversityofSzeged,Szeged,Hungary
bdicomLABDentalLtd.,Szeged,Hungary
cDepartmentofBiomaterialsScienceandTurkuClinicalBiomaterialsCenter–TCBC,InstituteofDentistry, UniversityofTurku,Turku,Finland
dResearchDevelopmentandProductionDepartment,StickTechLtd–MemberofGCGroup,Turku,Finland
eCityofTurku,WelfareDivision,Turku,Finland
a r t i c l e i n f o
Articlehistory:
Availableonlinexxx
Keywords:
Premolarteeth
Endodonticallytreatedteeth Shortfiber-reinforcedcomposite Fatiguesurvival
Bioblocktechnique
a bs t r a c t
Objectives.Theaimwastoinvestigatethefatiguesurvivalandmarginal-gapinsidetheroot- canalofendodonticallytreated(ET)premolarsreinforcedbyvariousfiber-reinforcedpost- corecomposites(FRCs).Moreover,composite-curingatdifferentdepthsinthecanalwas evaluated.
Methods.170intactupper-premolarswerecollectedandrandomlydividedintotengroups(n
=15).Onegroupservedascontrol(intact-teeth).AfterendodonticprocedurestandardMO cavitieswerepreparedandrestoredwithdifferentpost-corefiber-reinforcedmaterialsand designs.Three-group(A1-A3)wererestoredwitheitherpackableandflowableshortfiber- reinforcedcomposite(SFRC)coreorconventionalcomposite-core.Two-group(B1-B2)were restoredwithSFRCsasshortpost(3mm)andcore.Four-group(C1-C4)wererestoredwith SFRCsaspost(6mm)andcorewithorwithoutunidirectionalFRCposts(individually-made orconventional).Aftercompletingtherestorations,teethfromGroupC1-C4(n=5/group) weresectionedandstained.Specimenswereviewedunderastereo-microscopeandtheper- centageofmicrogapswithintheroot-canalwascalculated.Fatigue-survivalwasmeasured usingacyclic-loadingmachineintherestofthespecimens.
Results.ApplicationofflowableSFRCasluting-corematerialwithindividually-madeFRC post(GroupC3)didnotdifferfromintact-teethregardingfatigue-survival(p>0.05).The restofthegroupsproducedsignificantlylowersurvival(p<0.05)comparedtointact-teeth.
Post/corerestorationsmadefrompackableSFRC(GroupC1)hadalowermicrogap(19.1%) attheexaminedinterphaseintheroot-canalthanothergroups.
Significance.TherestorationofETpremolarswiththeuseofindividually-madeFRCpostand SFRCasluting-corematerialshowedpromisingachievementregardingfatigue-resistance andsurvival.
©2020TheAcademyofDentalMaterials.PublishedbyElsevierInc.Allrightsreserved.
∗ Correspondingauthorat:DepartmentofBiomaterialsScience,InstituteofDentistryandTCBC,UniversityofTurku,Turku,Finland.
E-mailaddress:sufgar@utu.fi(S.Garoushi).
https://doi.org/10.1016/j.dental.2020.11.026
0109-5641/©2020TheAcademyofDentalMaterials.PublishedbyElsevierInc.Allrightsreserved.
Pleasecitethisarticleinpressas:FráterM,etal.Fatiguebehaviorofendodonticallytreatedpremolarsrestoredwithdifferentfiber-reinforced
1. Introduction
Caries,traumaand cavitypreparationmaycausetoomuch lossofcoronaltoothstructure,whichisamajorchallengeto thecliniciansduringtherestorationofrootcanaltreated(RCT) teeth[1].Asaresultofloststructuralintegrity,RCTteethare weakand reveallimitedresistancetofracture [2,3]. Thisis mostlycriticalintheinstanceofRCTpremolars, asseveral investigationsreporting ahigh fracture incidenceforthese teeth, especially in the upper arch [4–6]. Upper premolars are subjected to a combination ofcompressive and shear- ingforces,whichdrivesthemparticularlypronetofracture [7].Themarginalridgeslossleadsthisevenmorenoticeable.
Reehet al., clearly showed that the lossofmarginal ridge integrityresultedinconsiderablelossofstiffness[3,8].While astandardized MOD(mesio-occlusal-distal) cavityprepara- tion in upper premolars was proved to lead in mean loss of63% inrelative cuspalstiffness [9], the lossof onlyone marginalridgeresultedinalossofonly46%inelativecus- palstiffness[10].Therefore,intracoronalreinforcementofRCT premolarsisessentialtodefendthemagainstfracture[7,11].
Sincethe1990s,fiber-reinforcedcomposite(FRC)postshave been used with increasing frequency to restore RCT teeth withexcessive lossofcoronaltoothstructure[12].Thesole aimofthisapproachistoinhancetheretentionofthecore build-up material. Many researchers reported that using a postintoRCTpremolarsconsiderablyimprovedtheirfracture resistance[13–16],though,otherresearchersjustmanagedto confirmthebeneficialeffectofplacingapostonthefracture modeofsuchpremolarteeth[17–19].Thiswasalsoapproved byTropeetal.[20],andZicarietal.[21],whoassumedthat placementofFRCpostdoesnotreallyenhanceorreinforce thegiventooth. Thiscouldbecaused bymultiplereasons, namelythepossibleweakeningoftherootduringthepost spacepreparation[21–23],theinaccuratefitofthepostdue totheirregulargeometryandcrosssectionoftherootcanal [24,25],ortheinabilityofthepostmaterialtoadequatelybond tothelutingorcorebuild-upmaterial[26,27].
Applyingshortfiber-reinforcedcomposites(SFRC) inside therootcanalhasbeensuggestedbymanyauthors[28–30].
Inthe Bioblock technique,both thecoronal cavityand the root canal are filled by packable SFRC in 4−5 mm thick horizontal increments[30,31]. From our previous research, premolarteethrestoredwiththeBioblocktechniqueshowed significantlyhigherfractureresistancecomparedtotheones restoredwithanFRCpost[31].In2019,theflowableversion ofSFRCwasreleasedwiththepromiseofeasyversatilityor adaptabilityinlimitedspaces(e.g.rootcanals).Inourlatest study,apexifiedanteriorteethrestoredwiththeBioblocktech- niqueusingtheflowableSFRCdidnotdiffersignificantlyfrom theintactteeth(controlgroup)intermsofsurvival,whereas therestofthetestedgroupshadsignificantlylowersurvival ratescomparedtothecontrolgroup[31].
Thequestionariseswhetheronemayusejustanyversion ofSFRCtorestore RCTpremolarteethwithmesio-occlusal (MO)cavities or long fibers (in the form ofFRC posts) are preferable.Thepurposeofthislaboratoryinvestigationwasto evaluatethefatigueresistanceandfailuremodeofRCTpre- molarwithMOcavitiesrestoredbydifferentdirecttechniques
withFRCmaterials.Furthermore,adaptationwithintheroot canalandcuringqualityatdifferentdepthswerestudiesfor eachtechnique.
2. Materials and methods
ThestudywasapprovedbytheEthicsCommitteeoftheUni- versityofSzeged,andwasdesignedinaccordancewiththe declarationofHelsinki.
Onehundredseventyupperpremolarteeth,extractedfor periodontalororthodonticcauseswereusedforthisresearch.
Thenewlyextractedpremolarsweredirectlyinsertedin5.25%
NaOClfor5minandstoredin0.9%salinesolutionatroom temperature. Teethwere usedduring8weeksafterextrac- tion.Attimeofspecimenpreparationhandscalerwasused toremovethesofttissuecoveringtherootsurface.Theteeth selection criteria were absence of caries, cracks, previous endodontictreatments,postsorcrowns,rootresorptionsand obvious accessorycanals.Radiographsfromdifferentdirec- tionsforallteethweretakenandexaminedtoevaluatethe number of existing canals and the root integrity. In order to standardize the test set-up, all premolars used in this reasearchhad onerootcanalwithacurvatureofless than 5◦, evaluated by Schneider’stechnique [32], and premolars witharootlengthof15±1mmandequalmesiodistaland bucco-lingualdimensions(±10%)were selected. 90%ofthe premolars ranged9–10mm insize,assessedatthe widest bucco-lingualdimension,andtherestmeasuredteethwere 6.5–8mm.Fromthemesio-distaldimension,90%oftheteeth ranged7–7.5mm,andtherestwere6.5–8mm.
Teethwererandomlydividedovertentestgroups,where four groups(GroupC1-C4)containedof20 specimenseach, andtherestofthegroupsonlycontaining15specimen.One groupcontaining15teethwasleftintacttoserveascontrol.
ClassII.MOcavitypreparationandlateronrootcanaltreat- mentwasconductedbythesametraineddentalpractitioner intherestofthegroups(GroupA1-A3,B1-B2andC1-C4).
2.1. Specimenpreparation
AstandardizedMOcavitywaspreparedonteethusingaround end paraleldiamondbur(883H.146.016FG-BrasselerUSA Dental, Savannah,GA) withwatercoolantsothat thebuc- copalatalwidthoftheocclusalisthmuswasonethird,and the proximalboxwidthwas twothirdsofthebuccopalatal width ofthecrown.Thegingivalfloorwas prepared1mm abovethecemento-enameljunction(CEJ).Allinternalangles wereroundedandthecavosurfacemarginswereat90◦.After finalizingtheMO cavitypreparation,accesscavityprepara- tionwasperfromedwitharound-enddiamondbur(850−014 MSSWhite,Lakewood,NJ,USA)withwatercoolingandroot canaltreatmentwasmadeinthepreparedteeth.Theworking lengthwascreated withthedirectmethodbysubtracting1 mmfromtherealrootlengthdefinedbyintroducinganum- ber10K-file(Maillefer-Dentsply,Ballaigues,Switzerland)until it was visible throughthe apical foramen. Therootcanals werepreparedusingrotaryProTaperUniversalfiles(Dentsply, Maillefer, Ballaigues, Switzerland). The ProTaper sequence (S1,S2,F1,F2)wasusedforthepreparationattheworking
Pleasecitethisarticleinpressas:FráterM,etal.Fatiguebehaviorofendodonticallytreatedpremolarsrestoredwithdifferentfiber-reinforced designs.DentMater(2020),https://doi.org/10.1016/j.dental.2020.11.026
ARTICLE IN PRESS
DENTAL-3689; No.ofPages12
dental materials xxx (2020)xxx–xxx
3
length.Irrigationwasdoneaftereveryinstrumentwith2ml of2.5%NaOCl solutionand the canalspace was saturated withirrigant during the instrumentation phase. After root canalcleaningandshaping,therootsweredriedusing96%
alcoholandpaperpoints.Rootcanalobturationwasmadeby matchedsingle-coneobturationwithamastercone(F2gutta- percha,Maillefer-Dentsply,Ballaigues,Switzerland)andsealer (AHplus;DentsplyDeTreyGmbH,Konstanz,Germany).The guttaperchawascutbacktotheleveloftheorificeandthe accesscavitywastemporarilyfilledwithFujiTriagePink(GC Europe,Leuven,Belgium).FujiTriagePinkwasappliedtothe apicalpartoftherootinordertopreventleakagethroughthe apex.Theteethwerestoredwetinanincubator(mco-18aic, Sanyo,Japan)foroneweek(at37◦C,100% relativehumid- ity).Afterthisthetemporarymaterialwasremovedandthe MOcavity,includingtheaccesscavitywasrefreshenedwitha diamondbur.
InGroupA1-A3therootcanalwasnolongerinvadedbyany preparationandteethwererestoredwithMOfillingwithout anyradicularreinforcement.InGroupB1-B2averyshallow postspacepreparationwascarriedoutbya1.2GCFiberPost drilltoadepthof3mmapicalfromtherootcanalorifice.In GroupC1-C4postspacepreparationwascarriedoutbya1.2 GCFiberPostdrilltoadepthof6mmapicalfromtherootcanal orifice.Aftercuttingbackthegutta-percha,therootcanalwas washedwithchlorhexidineanddriedwithpaperpoints.
Allspecimenhadthesameadhesivetreatment.Tofflemire (1101C0.035,Hawe-Neos,Italy)matrixbandwasappliedprior totheadhesivetreatmentofthecavityandtherootcanal,the enamelwasselectivelyacid-etchedwith37%phosphoricacid for15sandwashedwithwater.Thecoronalcavityandthe rootcanalwererinsedwith2mlofwateranddriedwithpaper pointsandair.Adual-cureone-stepself-etchadhesivesystem (G-PremioBondandDCA,GCEurope,Leuven,Belgium)was usedforbondingprocedureaccordingtothemanufacturer’s instructionsusingamicrobrush-Xdisposableapplicator(Pen- tron Clinical Technologies, LLC, USA). Extra adhesive was eliminatedbysuction drying(EvacuationTip–Starryshine, Anaheim, CA,USA)within0.5cm from theocclusal cavity (withoutcontact).Theexcessadhesiveresinatthebottomof thecanalwaseliminatedusingapaperpoint.Theadhesive waslight-curedfor60susinganOptilux501quartz-tungsten- halogenlight-curingunit(KerrCorp.,Orange,CA,USA).The light-curingtipwasalwayslocatedinclosecontact(1−2mm) withthetoothsurface.Theaveragepowerdensityofthelight source,measuredwithadigitalradiometer(Jetlitelighttester;
J.MoritaUSAInc.Irvine,CA,USA)beforethebondingproce- dure,was840±26.8mW/cm2.Afterlight-curingtheadhesive, themissinginterproximalwallswerebuild-upwithconven- tionalcomposite(G-aenialPosteriorPJ-E,GCEurope,Leuven, Belgium)usingthecentripetaltechnique,thustransforming theMOcavityintoaclassI.cavity.Thisinterproximalwall waslightcuredfor40s.
Ninedifferenttechniqueswereusedtorestorethespeci- mensinGroupA1-C4.(Fig.1):
GroupA1:ThecavitieswererestoredwithpackableSFRC (everXPosterior, GCEurope, Leuven, Belgium) appliedin a bulk-filltechnique.Thematerialwasplacedinsingleincre- mentaccordingtotheanatomyofthedentine,leaving1.5-2 mmocclusally forthe final compositelayersas prescribed
by the manufacturer.TheSFRC incrementwas light cured fromtheocclusalsurfacefor40s.Thelastocclusallayerwas conventionalcompositematerial(G-aenialPosteriorPJ-E)cov- eringtheSFRC.
GroupA2:ThecavitieswererestoredwithflowableSFRC (everXFlow,GCEurope,Leuven,Belgium)appliedinabulk- filltechnique.Thematerialwasplacedinsingleincrement accordingtotheanatomy ofthedentine, leaving1.5-2mm occlusallyforthefinalcompositelayersasprescribedbythe manufacturer.TheSFRCincrementwaslightcuredfromthe occlusalsurfacefor40s.Thelastocclusallayerwasconven- tionalcompositematerialcoveringtheSFRC.
Group A3:Thecavities were restoredwith conventional composite material (G-aenial Posterior) applied with an oblique incrementaltechnique. Thematerialwasplacedin consecutive2mmthickincrements.Eachincrementwaslight curedfromtheocclusalsurfacefor40s.
GroupB1:Thecavitiesincludingthe3mmdeeppostspace wererestoredwithpackableSFRCappliedinahorizontallay- ering technique. The materialwas placed in 2increments (approx.4mmthick each)accordingtotheanatomyofthe dentine. Thelightcuringofthe layersand coveringwitha finalocclusallayerofcompositematerialwasperformedasin GroupA1.
GroupB2:Thecavitiesincludingthe3mmdeeppostspace wererestoredwithflowableSFRCthesamewayasdescribed inGroupB1.
GroupC1:Thecavitiesandthe6mmdeeppostspacewere reconstructedwiththeBioblocktechniquedescribedbyFráter etal.,[30]buildingadirectlayeredpostandcorefrompackable SFRC.Anapprox.4mmthickincrementofusingamicrobrush- X disposableapplicator(PentronClinicalTechnologies,LLC, USA).AlighttransmittingFRCpost(1.2mmGCFiberpost, GCEurope,Leuven,Belgium)wasinsertedintothepostspace toaidthetransmissionofthelighttotheapicallypositioned layers.The‘lighttransmitting’postwaswithdrawnwith0.5–1 mmfromthesurfaceoftheuncuredSFRClayernottohave directcontactwithit.Thisapicallayerwaslightcuredthrough thefiberpostfor80s.Therestofthecavitywasrestoredas describedinGroupA1.
GroupC2:Thecavitiesandthe6mmdeeppostspacewere restored withthe Bioblocktechnique withtheuse offlow- ableSFRC.Thecoronalportionofthecavitywasrestoredas describedinGroupA2
Group C3:Theteethreceived anindividually-madeuni- directional FRC post (everStick Post, GC Europe, Leuven, Belgium).Beforetheadhesivetreatment,thepostsof1.2mm diameterwastriedinandcuttoalength2mmbelowthelevel oftheocclusalcavitymarginswithasterilescrissors.Lutingof thepostsandthecorebuild-upwasperformedwithflowable SFRC.FlowableSFRCwasappliedinanapprox.4mmthick layerintothepostspace.Afterinsertionofthepost,lightcur- ingwasperformedfor60s.Thecoronalportionofthecavity wasrestoredasdescribedinGroupA2.
GroupC4:Theteethreceivedaconventionalunidirectional FRCpost(GCFiberpost,GCEurope,Leuven,Belgium).Before the adhesive treatment, the conventional translucent FRC postsof1.2mmdiameterwastriedinandcuttoalength2mm belowtheleveloftheocclusalcavitymarginswithawater- cooleddiamonddisc(Isomet2000;BuehlerLtd.,LakeBluff,IL,
Pleasecitethisarticleinpressas:FráterM,etal.Fatiguebehaviorofendodonticallytreatedpremolarsrestoredwithdifferentfiber-reinforced Fig.1–Shematicfigurerepresentingthetestgroups(GroupA1-C4).Gr.A1:PackableSFRCcore;Gr.A2:FlowableSFRCcore;
Gr.A3:Conventionalcompositecore;Gr.B1:PackableSFRCdirectlylayeredaspost(3mm)andcore;Gr.B2:FlowableSFRC directlylayeredaspost(3mm)andcore;Gr.C1:PackableSFRCdirectlylayeredaspost(6mm)andcore;Gr.C2:Flowable SFRCdirectlylayeredaspost(6mm)andcore;Gr.C3:Individually-madeunidirectionalFRCpostlutedbyflowableSFRC;Gr.
C4:ConventionalunidirectionalFRCpostlutedbyflowableSFRC.
USA)andcleanedwithalcoholaftertryin.Thepostsreceived silanizationofthesurface(CeramicPrimer,GCEurope,Leu- ven,Belgium)followingthemanufacturer’srecommendation.
Aftersilanization,thepostsurfacewasbondedwiththesame bondingagent usedforthe cavity. Luting oftheposts and thecorebuild-upwasperformedwithflowableSFRC.Flow- ableSFRCwasappliedinanapprox.4mmthicklayerintothe postspace.Afterinsertionofthepost,lightcuringwasper- formedfor60s.Thecoronalportionofthecavitywasrestored asdescribedinGroupA2.
Finally,forallrestoredspecimens,glycerinegel(DeOxGel, UltradentProducts Inc.,Orange, CA,USA)was appliedand finalpolymerizationfromeachsidefor40swasperformed.
Therestorationswerefinishedwithafinegranulardiamond burr(FG7406-018,JetDiamonds,USAandFG249-F012,Horico, Germany)andaluminumoxidepolishers(OneGlossPSMidi, ShofuDentalGmbH,Ratingen,Germany).
2.2. Mechanicalloadingofthespecimen
Therestoredspecimenswerestoredindistilledwaterat37
◦C for a week. To simulate the periodontal ligament, the
root surface of each tooth was coated with a layer ofliq- uidlatexseparatingmaterial(Rubber-Sep,Kerr,Orange,CA) priortoembedding.Specimenswereembeddedinmethacry- lateresin(Technovit4004,Heraeus-Kulzer)at2mmfromthe cementoenameljunction(CEJ)tosimulatethebonelevel.For mechanicaltesting,therestored specimensweresubmitted toanacceleratedfatigue-testingprotocol[31]byahydraulic testing machine (Instron ElektroPlus E3000, Norwood, MA, USA) at an angle of 135 degrees to the long axis of each tooth.Testingwascarriedoutintwoparts.Duringthefirst part oftesting (simulation ofnormalforces) cyclicisomet- ricloadingwasappliedonthetriangularridgeofthebuccal cuspofthetoothusingaround-shapedmetallictip(witha diameter of 5mm). Thepalatal cusp was slightly reduced to aid the propoer positioning of the testing tip. A cyclic loadwasappliedatafrequencyof5Hz,startingwithgrad- uallyincreasingstaticloadingtill100Nin5s,followedby cyclic loadingin100N steps,up to500 N,5000cycles per step.Thespecimenswere loadeduntilfractureoccurred or 25,000 cycles were reached. The total number of survived cycleswererecordedforeachspecimenforthesurvivalanal- yses.
Pleasecitethisarticleinpressas:FráterM,etal.Fatiguebehaviorofendodonticallytreatedpremolarsrestoredwithdifferentfiber-reinforced designs.DentMater(2020),https://doi.org/10.1016/j.dental.2020.11.026
ARTICLE IN PRESS
DENTAL-3689; No.ofPages12
dental materials xxx (2020)xxx–xxx
5
The specimens that survived 25,000 cycles were then loaded withextremelyhigh forces simulatingparafunction (clenchingorbruxism).Duringthispartofthetesting,cyclic isometricloadingwascontinued.Cyclicloadwasappliedat a frequency of 5Hz, continuing with gradually increasing staticloadingupto600Nin5s, followedbycyclicloading in100Nsteps,upto1000N,5000cyclesperstep.Thespeci- menswereloadeduntilfractureoccurredor30,000cycleswere reached(withinthissecondphase).Thetotalnumberofsur- vivedcycleswererecordedforeachspecimenforthesurvival analyses.
Thefailed specimenswere visually examined under an opticalmicroscopeforthetype,locationanddirectionoffail- ure,withtwo-examineragreement.AccordingtoScottiand co-workers,adistinctionwasmadebetweenrepairableand irrepairablefractures,wherearepairablefractureisabovethe CEJ,meaningthatincaseoffracture,thetoothcanberestored, whileanirrepairablefractureextendsbelowtheCEJandthe toothislikelytobeextracted[33].
2.3. Microgapdetreminationtest
Fourgroups(C1-4),eachconsistingof5endodonticallytreated andrestoredteeth,wereinvestigatedinthemicrogapdetrem- inationtest.Theteeth(n=20)wererestoredinthesameway asmentioned earlier.Teethweresectioned mid-sagitallyin themesio-distalplaneusingaceramiccuttingdisc operat- ingataspeedof100rpm(Struers,Glasgow,Scotland)under watercooling.Ineach group,oneofthe sectionedrestora- tionthatcontainsthepostwasfurthergrindandpolishusing
#4000-gritsiliconcarbidepapersat300rpmunderwatercool- ingusinganautomaticgrindingmachine(Rotopol-1;Struers, Copenhagen,Denmark).Then,sectionedteethwerepainted withpermanentmarker,andpolishgentlyforfewseconds.
Thedye penetration along post/core margins of each sec- tionwasevaluatedindependentlyusingastereo-microscope (HeerbruggM3Z,Heerbrugg,Switzerland)atamagnification of6.5xandtheextentofdyepenetrationwasrecordedinmm asapercentageofthetotalmarginlength[34].
2.4. Microhardnesstest
Microhardnessoflutingcompositeinsidethecanalwasmea- suredusingaStruersDuraminhardnessmicroscope(Struers, Copenhagen,Denmark)witha40objectivelensandaloadof 1.96Nappliedfor10s.Eachsectionedrestorationwassub- jected to 5indentations on the top (coronal part) and the bottom(apicalpart)ofthecanalforindicationofpolymeriza- tion[35,36].Thediagonallengthimpressionsweremeasured andVickersvalueswereconverted intomicrohardnessval- uesbythemachine.Microhardnesswasobtainedusingthe followingequation:
H= 1854.4×P d2
whereHisVickershardnessinkg/mm2,Pistheloadingrams anddisthelengthofthediagonalsinm.
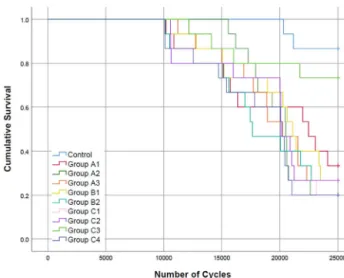
Fig.2–Fatigueresistancesurvivalcurves(Kaplan-Meier survivalestimator)foralltestedgrouploadedwithaforce ofmagnitude100-500N.
Fig.3–Fatigueresistancesurvivalcurves(Kaplan-Meier survivalestimator)foralltestedgroupsloadedwithaforce ofmagnitude600-1000N.
2.5. Statisticalanalysis
StatisticalanalyseswereperformedinSPSS21.0(IBM,USA).
Groupsweredefinedaccordingtothemethodofrestoration(or thelackthereofforthecontrolgroup).Thenumberofsurvived cycleswasanalyzeddescriptivelyforeachgroupandwiththe Kaplan-Meiermethodacrossthegroups(withtheBreslowtest forthe pairwiseanalyses).Thefrequencyofrestorable and non-restorabefractureswascalculatedforeachgroup.
3. Results
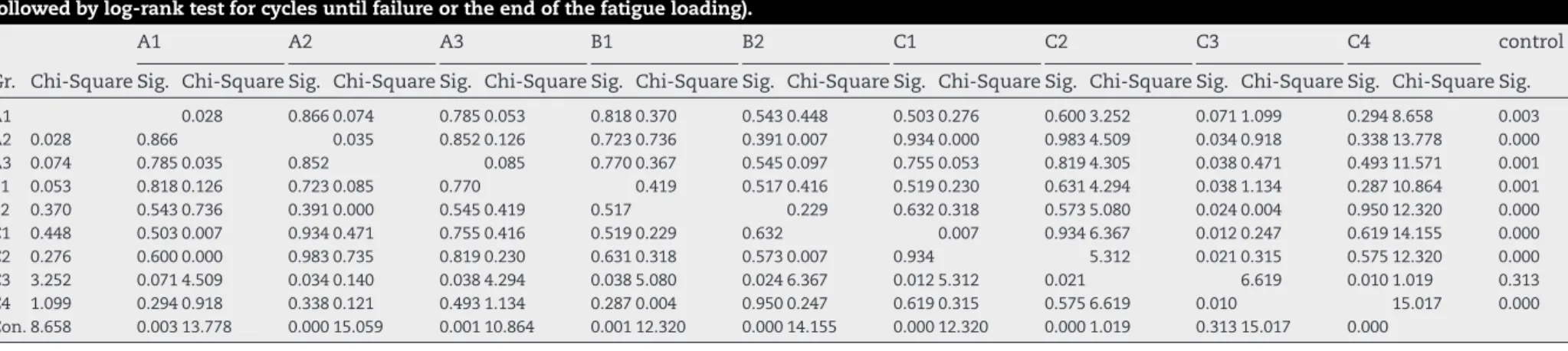
TheKaplan–Meiersurvivalcurvesforthetestsimulatingnor- mal(100−500N)andparafunctional(600−1000N)forcesare displayedinFigs.2and3respectively.Table1presentsthep valuesforgroup-wisecomparisonsinthetestsimulatingnor-
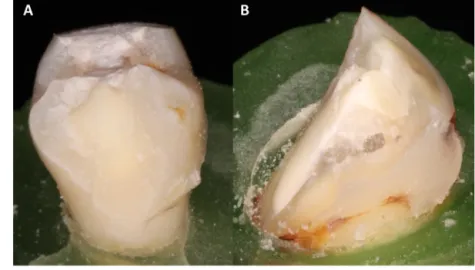
Pleasecitethisarticleinpressas:FráterM,etal.Fatiguebehaviorofendodonticallytreatedpremolarsrestoredwithdifferentfiber-reinforced Fig.4–Photographsofrepairable(A)andirrepairable(B)fracturepatternofthetestedspecimens.
malforces,whileTable2presentsthepvaluesforgroup-wise comparisonsinthetestsimulatingparafunctionalforces.
Inthetestsimulatingnormalforces thesurvivalrateof GroupC3wasnotshowingsignificantdifference(p>0.05)from GroupA1orthecontrolgroup(intactteeth).Therestofthe groupshadsignificantlylowersurvivalratescomparedtoboth GroupC3andthecontrolgroup.
Inthetestsimulatingparafunctionalforcesforthespeci- menssurvivedthefirstphaseofmechanicaltesting(n=54), the survivalrate ofthe control group showed significantly highersurvival(p<0.05)comparedtotherestofthetested groups.Therestoredgroupspresentinthesecondphaseof thetestdidnotdiffersignificantly(p>0.05)fromeachother intermsofsurvival.
Allrestoredgroupsshoweddominantlyirrepairablefrac- tures, whereas only the control group presented almost exclusivelyrepairablefractures(Table3andFig.4).
The average values with SD of microgap percentage at post/core–toothinterfaceoffourgroups(C1-C4)areillustrated inFig.5.Valuesrevealedthatpost/corerestorationsmadeof directlylayeredpackableSFRC(GroupC1)hadalessmicrogap (19.1%)thanothertestedgroups.While,GroupC3exhibited thehighestnumberofmicrogap(55.9%)atthestudiedinter- phasewithintherootcanal(Fig.5).
Concerningthemicrohardnessvaluesforthepackableand flowableSFRCsatthebottom(apical)oftherootcanal,flow- ableSFRC(C2-C4)showedhighermicrohardnessvalues(56.9 VH)aswellaslowerdifferenceamongthemicrohardnessval- ues atthecoronal andatthe apicalpart ofthe rootcanal (Fig.6).
4. Discussion
Oneofthemaingoalsofpost-endodonticrestorationofRCT teethisrestoringlostresistancetomasticatoryload[37].In thisinvestigation,upperRCTpremolarswithMOcavitieswere selectedastheypresentanunfavorableanatomyincrownto rootratioand crownvolume,whichmakesthematgreater risktocuspfracturescomparedtootherposteriorteethwhen subjectedto occlusalload[13]. Furthermore,premolarsare
Fig.5–Meanpercentageofmicrogapobservedindifferent groupsfromtotalpost/core-toothinterfacelengthafter staining.Verticallinesrepresentstandarddeviation.
exposedtomoredetrimentallateralforcesthanmolarsdur- ing mastication,namelyacombination ofcompressive and shearforcesthatraisesthepossibilityofcuspfracture[38].The testedspecimensloadedwithanangle(45degreetothelong axisofthetooth),whichseemstobetheworst-casescenario inregardstothefractureresistanceofRCTteethasdescribed byWandscherandhiscolleagues[39].
According toFerrarioet al.,the normalbitingforce that developsduringasingletoothbiteisapproximately250–290 Nforthefirstandsecondpremolarsinhealthyyoungmale adults [40].This isinaccordance with the findings ofJan- tarahetal.,whoreportedthenormalbitingforceformaxillary premolarstobeintherangebetween100–300N[41].How- ever,higherbitingforceshavetobepredictedinindividuals withfunctionaldisturbances,suchasclenchingorbruxism where biting force can beas high as 520–800 N[42,43]. It wasonthebasisofthesepublishedvaluesthatwedivided our testprotocol into2phases, wherethe firstphasesim- ulated normal biting forces (up to 500 N) and the second phase simulatedextremelyhigh forces(up to1000N).The
Pleasecitethisarticleinpressas:FráterM,etal.Fatiguebehaviorofendodonticallytreatedpremolarsrestoredwithdifferentfiber-reinforceddesigns.DentMater(2020),https://doi.org/10.1016/j.dental.2020.11.026
AR TICLE IN PRESS
DENTAL-3689;No.ofPages12dentalmaterialsxxx(2020)xxx–xxx
7
Table1–pvaluesofpairwiselog-rankpost-hoccomparisonsamongtestedgroupsloadedwithaforceofmagnitude100-500N(Kaplan-Meiersurvivalestimator followedbylog-ranktestforcyclesuntilfailureortheendofthefatigueloading).
A1 A2 A3 B1 B2 C1 C2 C3 C4 control
Gr. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig.
A1 0.028 0.8660.074 0.7850.053 0.8180.370 0.5430.448 0.5030.276 0.6003.252 0.0711.099 0.2948.658 0.003
A2 0.028 0.866 0.035 0.8520.126 0.7230.736 0.3910.007 0.9340.000 0.9834.509 0.0340.918 0.33813.778 0.000
A3 0.074 0.7850.035 0.852 0.085 0.7700.367 0.5450.097 0.7550.053 0.8194.305 0.0380.471 0.49311.571 0.001
B1 0.053 0.8180.126 0.7230.085 0.770 0.419 0.5170.416 0.5190.230 0.6314.294 0.0381.134 0.28710.864 0.001
B2 0.370 0.5430.736 0.3910.000 0.5450.419 0.517 0.229 0.6320.318 0.5735.080 0.0240.004 0.95012.320 0.000
C1 0.448 0.5030.007 0.9340.471 0.7550.416 0.5190.229 0.632 0.007 0.9346.367 0.0120.247 0.61914.155 0.000
C2 0.276 0.6000.000 0.9830.735 0.8190.230 0.6310.318 0.5730.007 0.934 5.312 0.0210.315 0.57512.320 0.000
C3 3.252 0.0714.509 0.0340.140 0.0384.294 0.0385.080 0.0246.367 0.0125.312 0.021 6.619 0.0101.019 0.313
C4 1.099 0.2940.918 0.3380.121 0.4931.134 0.2870.004 0.9500.247 0.6190.315 0.5756.619 0.010 15.017 0.000
Con.8.658 0.00313.778 0.00015.059 0.00110.864 0.00112.320 0.00014.155 0.00012.320 0.0001.019 0.31315.017 0.000
Table2–pvaluesofpairwiselog-rankpost-hoccomparisonsamongtestedgroupsloadedwithaforceofmagnitude600-1000N(Kaplan-Meiersurvivalestimator followedbylog-ranktestforcyclesuntilfailureortheendofthefatigueloading).
A1 A2 A3 B1 B2 C1 C2 C3 C4 control
Gr. Chi-Square Sig. Chi-Square Sig. Chi-Square Sig. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig. Chi-SquareSig.
A1 0.022 0.8810.235 0.6283.938 0.0470.928 0.3361.000 0.3170.928 0.3360.029 0.8660.184 0.6680.022 0.000
A2 0.022 0.881 0.533 0.4650.533 0.4650.533 0.4650.429 0.5130.533 0.4650.006 0.9380.429 0.5138.008 0.000
A3 0.235 0.6280.533 0.465 1.391 0.2380.000 1.0000.471 0.4930.735 0.3910.140 0.7080.121 0.72815.059 0.000
B1 3.938 0.0470.533 0.4651.391 0.238 0.735 0.3910.500 0.4800.750 0.3860.973 0.3242.207 0.1375.255 0.000
B2 0.928 0.3360.533 0.4650.000 1.0000.735 0.391 0.000 1.0000.000 1.0000.065 0.7990.000 1.0008.290 0.004
C1 1.000 0.3170.429 0.5130.471 0.4930.500 0.4800.000 1.000 0.032 0.8580.624 0.4300.409 0.5227.877 0.005
C2 0.928 0.3360.533 0.4650.735 0.3910.750 0.3860.000 1.0000.032 0.858 0.952 0.3290.500 0.4809.587 0.002
C3 0.029 0.8660.006 0.9380.140 0.7080.973 0.3240.065 0.7990.624 0.4300.952 0.329 0.137 0.71214.569 0.000
C4 0.184 0.6680.429 0.5130.121 0.7282.207 0.1370.000 1.0000.409 0.5220.500 0.4800.137 0.712 12.129 0.000
Con.17.069 0.0008.008 0.00515.059 0.0005.255 0.0228.290 0.0047.877 0.0059.587 0.00214.569 0.00012.129 0.000
Pleasecitethisarticleinpressas:FráterM,etal.Fatiguebehaviorofendodonticallytreatedpremolarsrestoredwithdifferentfiber-reinforced Fig.6–Microhardness(VH)meanvaluesforpackableand
flowableSFRCsatthetop(coronal)andbottom(apical)part oftherootcanal.ArrowsabovethecolumnsindicateVHof thisgroupdroppedbelow80%ofthecoronalpartvalue.
Verticallinesrepresentstandarddeviation.
latteraspectrequirestobetakenintoconsiderationbecause temporomandibulardisordersarehighlyprevalentinWestern societies[44].Occlusalloadisakeyfactorinthesuccessful treatmentofroot-filledteethanditiscrucialfortheclinician toknowifthepatienthasparafunctionalmovements[45].
Inourstudy,onlyspecimensrestoredwithanindividually- madeunidirectionalFRCpostlutedwithflowableSFRC(Group C3) showed significantly higher survival compared to the rest of the restored groups when exposed to normal bit- ing forces. The only exception was the Group A1, which did not differ significantly from the C3 group in terms of survival. The individually-made post used in Group C3 is made ofunidirectional fibers (E-glass) impregnated with a combination of bisphenol A-glycidyl methacrylate as the cross-linkedphaseandpolymethylmethacrylateasalinear phase,whichtogetherformasemi-interpenetratingpolymer network(semi-IPN)[46].Asthesemi-IPNstructurecontains both cross-linked and linear polymerphases, it ensures a stableadhesiontoresinmaterialsusedforluting.Logically, this could possiblyinfluence the fracture resistanceofthe restoration.InthestudyofDoshietal.,teethrestored with the individually-made FRC post presented higher fracture resistance compared to the ones restored with a conven- tionalFRCpost[47].Onthecontrary,inourpreviousstudy the individually-madeFRCpost didnot makeasignificant differenceinregardstofractureresistancecomparedtoacon- ventionalFRCpost[48].Itmustbenotedthatinthementioned study the teeth were decoronated premolar teeth(not MO cavities),andalsothelutingandcorebuild-upmaterialwas aconventionalparticulatefilleddual-cureresin,notafiber- reinforcedone.Thesamewasfoundinourlateststudywhere apexifiedanteriorteethwereused[31].Inthispresentstudy, thesuperior resistanceofthespecimensrestored withthe individually-madeFRCpostmightbeattributedtotheflow- ableSFRCusedforpostlutingandsubsequentcorebuild-up.
TheflowableSFRCformsaunitwiththeindividually-made
postduetothesemi-IPNpolymermatrixofthispost.Stud- ieshavedemonstratedincreasedbondstrengthbetweenthe individually-made FRCpost and compositeresin materials comparedtoconventionalFRCpost [26].Toourknowledge, flowableSFRChasnotbeenusedtolutepostsintorootcanals.
Thisindicationcouldbeimportantfromabiomimeticpointa view.FRCpostsusuallydonothaveaperfectfitinsidetheroot duetotheirregularanatomyandindividualcrosssectionof therootcanal.Asaresult,itisusuallythemechanicallyinfe- riorlutingmaterialthatfillsout thegapsbetweentheroot canalwallsand the post,actingasthe interfacialmedium betweenthem.Asdetrimentaltensilestressesoccuronthe surfacesoftherootcanalwalls,therestorativematerialplaced withtheintentionofstress-bearingshouldbeluteddirectly to them withclosecontact[49]. As highlightedby LeBell- Rönnlöfetal.,iftheconventionalFRCpostisinsertedinthe mostcentral partofthe post position(i.e.theneutralaxis ofthetooth),the postisnotideallyplacedwithrespectto biomechanics if reinforcement isthe intendedresults [49].
Beside their superior resistance in the normal force range (100−500N),specimensrestoredwiththeindividually-made FRCpostcombinedwithflowableSFRCdidnotshowstatis- ticallysignificant differencecomparedtocontrols(Table1).
Fiber-reinforced materials are increasingly used for crack- arrestingandreinforcementinhighstress-bearingareas.In theBioblocktechnique,SFRCisdirectlyandtightlyfittedtothe wallofrootcanal,excludingtheshortcomingsoftheusageof lutingcementorthebiomechanicallyimproperpositioningof theFRCpost,thustheoreticallyeliminatingalldamagingten- silestressescreatedwhentherestorationisloaded[30].This enablestheclinician tofillandrestoreany rootcanalwith irregularcrosssectiondeemednotidealforFRCpostinser- tion.WiththeBioblocktechnique,theamountoffiberscanbe maximizedalsointhecriticalcervicalareaofthetooth,which seemstobeimportantregardingfuturestressaccumulation [50].Notlessimportantly,theBioblocktechniqueminimizes the numberofinterfaceswithintherestoration-toothcom- plex, whichhas been shown to be beneficial as interfaces increases the amount ofstress withinthis unit [51].Inter- estingly,inthisstudyneitherthenormalBioblocktechnique (GroupC1),noritsmodification(extendingonly3mmintothe canal;GroupB1)achievedsurvivalcomparabletoGroupC3or intactteeth.Inoneofourpreviousstudies,theBioblocktech- niqueyieldedhigher fractureresistancecomparedtoteeth restoredwithaconventionalFRCpost.However,inthatstudy wetestedtherestorationofMODcavities inpremolarsand static loadingwas applied[30].Our currentfindings are in accordance withpreviousstudiesshowingthatrestorations prepared with the Bioblock technique failed toreach frac- tureresistanceorsurvivalcomparabletointactteeth,inMOD RCTpremolars[30]andapexifiedanteriorteeth[31],respec- tively.Theperformanceoffiberreinforcementreliesonmany factors,namelytheusedresins,thethickness,length,posi- tionandtheorientationoffibers,thefibersaspectratio,the adhesionofthepolymermatrixandfibers,andtheimpreg- nationofthefibersintotheresin[52].Thefiberaspectratio refers tothe lengthofthe fiber compared tothe diameter of the fiber (l/d). Thefiber aspectratio isof majorimpor- tanceinthecaseofmodernfiber-reinforcedmaterialssinceit affectsflexuralmodulus,tensilestrength,andthereinforcing
Pleasecitethisarticleinpressas:FráterM,etal.Fatiguebehaviorofendodonticallytreatedpremolarsrestoredwithdifferentfiber-reinforced designs.DentMater(2020),https://doi.org/10.1016/j.dental.2020.11.026
ARTICLE IN PRESS
DENTAL-3689; No.ofPages12
dental materials xxx (2020)xxx–xxx
9
Table3–Thedistributionoffracturepatternamongthetestedgroups(n=15).
Fracturepattern A1 A2 A3 B1 B2 C1 C2 C3 C4 Control
repairable 1 3 2 1 0 1 0 0 0 12
irrepairable 14 12 13 14 15 14 15 15 15 3
efficiencyofthematerial[53,54].WhilepackableSFRCcon- tainsmillimeter-longfibers,thefibersintheflowableSFRCare micrometer-long.Evenwiththeshorterfibersincorporatedin theflowableSFRC,thefiberaspectratioiswithintherangeof 30–94[55],thusofferingreinforcementtothematerialsand likelytotheadhereddental tissues.Curiously,theBioblock techniquedid notallowsuperiorsurvival comparedtothe othergroupsandwassignificantlyweakercomparedtointact teeth,evenwiththeflowableSFRC.Thisisagainstourpre- viousfindingsinanteriorapexifiedteethwheretheBioblock techniquewithflowableSFRCwastheonlytestedrestorative techniqueyieldedsurvivalcomparabletointactteeth[31].
Regardingthe fracturebehaviorand load-bearingcapac- ityofSFRCrestorations,Lassilaetal.,statedthattheoptimal thickness of the surface conventional composite over the SFRC-coreisbetween0.5–1mm[56].Assumingthatreinforce- mentroleoftheSFRC-coreisbuiltuponthemechanismofa crack-stopper,thelengthfromthesurfaceofthestressstart- ingpointtotheSFRC-coreisofimportance.Thus,theveneered conventional composite thickness might contribute to the crackpropagationandthe survivalrate ofthe restorations.
Thisisconsistentwithearlierinvestigationswhichshowed theimportanceofhowthickSFRCandconventionalsurface layersshouldbeapplied[57,58].
MostdentalpractitionersregularlyrestoreRCTupperpre- molarswithconventionalfiberposts,butthisapproachisa matterofdebate[4].Thereare studiestoindicatethatRCT upperpremolarswithout afiberpostshow similarfracture resistancetothoserestoredwithapost[59–61],whileother studiesshowedsuperiorresultswhenaconventionalFRCpost wasusedcomparedtoacompositefillingalone[62,63].Inour presentsetup,therewasnodifferencebetweenteethrestored withaconventionalcompositefillingalone(GroupA3)orwith aconventionalFRCpostandflowableSFRC(GroupC4).The survivalofthegroupsrestoredwiththelattertwotechniques wasalsosignificantlylowercomparedtointactteeth.Ourcur- rentfindingsarealsoinaccordancewiththoseofShahetal.
[37],and Nothdurftet al.[16],showingthatRCTpremolars withMOcavitiescannotbereinforcedwithacompositefilling only,astheseteethdonothavethesamefractureresistanceas intactteeth.Asfortestingintheextremeforcerange,noneof thetestedtechniquesallowedsurvivalcomparabletointact teeth.Thisisimportanttoconsiderwhentreatingpatients whocouldpossiblyoverloadtherestorationduetoclenching orbruxism.Regardingthefracturepatterns,allspecimensin allgroupsshowedpredominantlyirreparablefractures,except forthecontrolgroup,wherethefractureswerepredominantly reparable.
Consideringtheadaptationofthe usedmaterialswithin therootcanalappearestobeveryimportant,gapformation wasalsoevaluatedwitha microgapdetermingtestforthe packableandflowableSFRCs(Fig.5).ThepackableSFRC(Group C1)hadnotablygoodadaptationtothecanalwallsthanother testedgroups(C2-C4),whichwasinagreementwithourpre-
viousfindings[30,31].Thoughtheadaptationofthepackable SFRCtothecanalwallswasideal,voidswereseenwithinthe materialitself.Thesevoidscouldbeduetopoorcondensation ofthematerialinsidethetightenspace,orentrapmentofair whenapplyingthethickmaterialintothecanal.Theauthors’
opinionisthatthesevoidscouldcontributeinreducingthe shrinkage stress duringthe polymerization and this might decreasethemicrogapsatinterfaces.Infact,thishasbeensug- gestedalsoearlierwhentheinfluenceofFRCinregularfilling applicationwasstudied[64].
Inlinewithpreviousfindingsandduetothehighervolu- metricshrinkageoftheflowableSFRC,themicrogapformation attheexaminedinterphaseintherootcanalwithflowable SFRC(GroupC2-C4),wasnotsoperfect.
Microhardnesstestwascarriedoutinordertoassessthe curingofSFRCsinsidetherootcanal.Thedatarevealedthat SFRCs used in the coronal part of the canalhad superior microhardnesscomparedtotheapicalpartofthesamecanal, demonstratingenhancecuringduetohigherintensityoflight polymerization.Inthecrucialapicalpartofthecanal,flow- ableSFRC(C2-C4)showedhighermicrohardnessvaluesand alsolowerdifferencebetweenthemicrohardnessmeasured attheapicalandatthecoronalpartsoftherootcanal(Fig.6).
Thisisinlinewithprevious resultsshowingthatSFRCcan belight-curedinsidethecanal[29–31].Thisisresultingfrom boththetranslucencyofthematerialandthefactthattheran- domlyorientedfiberswithinitmayconductandscatterthe lightoverlongerdistances[65].Ithasbeenshownthatrefrac- tion indexofglassfibers and dimatehacrylateresin matrix duringitscuringphasebenefitslightscatteringandimproves photopolymerization[66].
Tomimicmoreclinicalenvironmentandtohaveperfect view ofrestorative material/design behavior under clinical conditions,fatiguesurvivalafterlong-termwaterstorageand thermalagingshouldalsobetakenintoconsideration.
5. Conclusion
TherestorationofETpremolarswiththeuseofindividually- made FRC post and SFRC as luting-core material showed promisingachievementregardingfatigue-resistanceandsur- vival.
references
[1] ZavattiniA,FeitosaVP,ManocciF,FoschiF,BabbarA,LuziA, etal.Bondingabilityofexperimentalresin-basedmaterials containing(ion-releasing)-microfillersappliedonwater-wet orethanol-wetrootcanaldentine.IntJAdhesAdhes 2014;54:214–23,
http://dx.doi.org/10.1016/j.ijadhadh.2014.06.007.
[2] Al-OmiriMK,MahmoudAA,RayyanMR,Abu-HammadO.
Fractureresistanceofteethrestoredwithpost-retained
Pleasecitethisarticleinpressas:FráterM,etal.Fatiguebehaviorofendodonticallytreatedpremolarsrestoredwithdifferentfiber-reinforced restorations:anoverview.JEndod2010;36(9):1439–49,
http://dx.doi.org/10.1016/j.joen.2010.06.005.
[3] ReehES,MesserHH,DouglasWH.Reductionintooth stiffnessasaresultofendodonticandrestorative procedures.JEndod1989;15(11):512–6,
http://dx.doi.org/10.1016/S0099-2399(89)80191-8.
[4] MohammadiN,KahnamoiiMA,YeganehPK,NavimipourEJ.
Effectoffiberpostandcuspcoverageonfractureresistance ofendodonticallytreatedmaxillarypremolarsdirectly restoredwithcompositeresin.JEndod2009;35(10):1428–32, http://dx.doi.org/10.1016/j.joen.2009.07.010.
[5] YamadaY,TsubotaY,FukushimaS.Effectofrestoration methodonfractureresistanceofendodonticallytreated maxillarypremolars.IntJProsthodont2004;17(1):
94–8.
[6] SorrentinoR,DiMauroMI,FerrariM,LeoneR,ZaroneF.
Complicationsofendodonticallytreatedteethrestoredwith fiberpostsandsinglecrownsorfixeddentalprostheses-a systematicreview.ClinOralInvestig2016;20(7):1449–57, http://dx.doi.org/10.1007/s00784-016-1919-8.
[7] OskoeePA,AjamiAA,NavimipourEJ,OskoeeSS,SadjadiJ.
Theeffectofthreecompositefiberinsertiontechniqueson fractureresistanceofroot-filledteeth.JEndod
2009;35(3):413–6,http://dx.doi.org/10.1016/j.joen.2008.11.027.
[8] WuY,CathroP,MarinoV.Fractureresistanceandpatternof theupperpremolarswithobturatedcanalsandrestored endodonticocclusalaccesscavities.JBiomedRes 2010;24(6):474–8,
http://dx.doi.org/10.1016/S1674-8301(10)60063-2.
[9] El-HelaliR,DowlingAH,McGinleyEL,DuncanHF,Fleming GJ.Influenceofresin-basedcompositerestorationtechnique andendodonticaccessoncuspaldeflectionandcervical microleakagescores.JDent2013;41(3):216–22,
http://dx.doi.org/10.1016/j.jdent.2012.11.002.
[10] PlotinoG,BuonoL,GrandeNM,LamorgeseV,SommaF.
Fractureresistanceofendodonticallytreatedmolars restoredwithextensivecompositeresinrestorations.J ProsthetDent2008;99(3):225–32,
http://dx.doi.org/10.1016/S0022-3913(08)60047-5.
[11] BelliS,ErdemirA,YildirimC.Reinforcementeffectof polyethylenefibreinroot-filledteeth:comparisonoftwo restorationtechniques.IntEndodJ2006;39(2):136–42, http://dx.doi.org/10.1111/j.1365-2591.2006.01057.x.
[12] ZicariF,DeMunckJ,ScottiR,NaertI,VanMeerbeekB.
Factorsaffectingthecement-postinterface.DentMater 2012;28(3):287–97,
http://dx.doi.org/10.1016/j.dental.2011.11.003.
[13] SoaresPV,Santos-FilhoPC,MartinsLR,SoaresCJ.Influence ofrestorativetechniqueonthebiomechanicalbehaviorof endodonticallytreatedmaxillarypremolars.PartI:fracture resistanceandfracturemode.JProsthetDent
2008;99(1):30–7,
http://dx.doi.org/10.1016/S0022-3913(08)60006-2.
[14] ScottiN,ScansettiM,RotaR,PeraF,PasqualiniD,BeruttiE.
Theeffectofthepostlengthandcuspcoverageonthe cyclingandstaticloadofendodonticallytreatedmaxillary premolars.ClinOralInvestig2011;15(6):923–9,
http://dx.doi.org/10.1007/s00784-010-0466-y.
[15] BitterK,NoetzelJ,StammO,VaudtJ,Meyer-LueckelH, NeumannK,etal.Randomizedclinicaltrialcomparingthe effectsofpostplacementonfailurerateofpostendodontic restorations:preliminaryresultsofameanperiodof32 months.JEndod2009;35(11):1477–82,
http://dx.doi.org/10.1016/j.joen.2009.07.026.
[16] NothdurftFP,SeidelE,GebhartF,NaumannM,MotterPJ, PospiechPR.Thefracturebehaviorofpremolarteethwith classIIcavitiesrestoredbybothdirectcomposite restorationsandendodonticpostsystems.JDent
2008;36(6):444–9,
http://dx.doi.org/10.1016/j.jdent.2008.03.004.
[17] QualtroughAJ,MannocciF.Tooth-coloredpostsystems:a review.OperDent2003;28(1):86–91.
[18] SoaresCJ,SoaresPV,deFreitasSantos-FilhoPC,CastroCG, MagalhaesD,VersluisA.Theinfluenceofcavitydesignand glassfiberpostsonbiomechanicalbehaviorof
endodonticallytreatedpremolars.JEndod2008;34(8):1015–9, http://dx.doi.org/10.1016/j.joen.2008.05.017.
[19] StocktonL,LavelleCL,SuzukiM.Arepostsmandatoryfor therestorationofendodonticallytreatedteeth?EndodDent Traumatol1998;14(2):59–63,
http://dx.doi.org/10.1111/j.1600-9657.1998.tb00810.x.
[20] TropeM,MaltzDO,TronstadL.Resistancetofractureof restoredendodonticallytreatedteeth.EndodDent Traumatol1985;1(3):108–11,
http://dx.doi.org/10.1111/j.1600-9657.1985.tb00571.x.
[21] ZicariF,VanMeerbeekB,ScottiR,NaertI.Effectoffibrepost lengthandadhesivestrategyonfractureresistanceof endodonticallytreatedteethafterfatigueloading.JDent 2012;40(4):312–21,
http://dx.doi.org/10.1016/j.jdent.2012.01.006.
[22] MeyenbergK.Theidealrestorationofendodontically treatedteeth-structuralandestheticconsiderations:a reviewoftheliteratureandclinicalguidelinesforthe restorativeclinician.EurJEsthetDent2013;8(2):238–68.
[23] AurélioIL,FragaS,RippeMP,ValandroLF.Areposts necessaryfortherestorationofrootfilledteethwithlimited tissueloss?Astructuredreviewoflaboratoryandclinical studies.IntEndodJ2016;49(9):827–35,
http://dx.doi.org/10.1111/iej.12538.
[24] Faria-e-SilvaAL,Pedrosa-FilhoCdeF,MenezesMdeS, SilveiraDM,MartinsLR.Effectofreliningonfiberpost retentiontorootcanal.JApplOralSci2009;17(6):600–4, http://dx.doi.org/10.1590/s1678-77572009000600012.
[25] D’ArcangeloC,CinelliM,DeAngelisF,D’AmarioM.The effectofresincementfilmthicknessonthepulloutstrength ofafiber-reinforcedpostsystem.JProsthetDent
2007;98(3):193–8,
http://dx.doi.org/10.1016/S0022-3913(07)60055-9.
[26] BellAM,LassilaLV,KangasniemiI,VallittuPK.Bondingof fibre-reinforcedcompositeposttorootcanaldentin.JDent 2005;33(7):533–9,
http://dx.doi.org/10.1016/j.jdent.2004.11.014.
[27] ChieruzziM,PaganoS,PennacchiM,LombardoG,D’ErricoP, KennyJM.Compressiveandflexuralbehaviouroffibre reinforcedendodonticposts.JDent2012;40(11):968–78, http://dx.doi.org/10.1016/j.jdent.2012.08.003.
[28] GaroushiS,VallittuPK,LassilaLV.Continuousandshort fiberreinforcedcompositeinrootpost-coresystemof severelydamagedincisors.OpenDentJ2009;3:36–41, http://dx.doi.org/10.2174/1874210600903010036.
[29] ForsterA,SáryT,BraunitzerG,FráterM.Invitrofracture resistanceofendodonticallytreatedpremolarteethrestored withadirectlayeredfiber-reinforcedcompositepostand core.JAdhesSciTechnol2016;31,1454–66.
https://doi.org/10.1080/01694243.2016.1259758.
[30] FráterM,LassilaL,BraunitzerG,VallittuPK,GaroushiS.
Fractureresistanceandmarginalgapformationofpost-core restorations:influenceofdifferentfiber-reinforced
composites.ClinOralInvestig2020;24(1):265–76, http://dx.doi.org/10.1007/s00784-019-02902-3.
[31] FráterM,SáryT,NémaV,etal.Fatiguefailureloadof immatureanteriorteeth:influenceofdifferentfiber post-coresystems.Odontology2020,
http://dx.doi.org/10.1007/s10266-020-00522-y.
[32] SchneiderSW.Acomparisonofcanalpreparationsin straightandcurvedrootcanals.OralSurgOralMedOral
Pleasecitethisarticleinpressas:FráterM,etal.Fatiguebehaviorofendodonticallytreatedpremolarsrestoredwithdifferentfiber-reinforced designs.DentMater(2020),https://doi.org/10.1016/j.dental.2020.11.026
ARTICLE IN PRESS
DENTAL-3689; No.ofPages12
dental materials xxx (2020)xxx–xxx
11
Pathol1971;32(2):271–5,
http://dx.doi.org/10.1016/0030-4220(71)90230-1.
[33] ScottiN,CoeroBorgaFA,AlovisiM,RotaR,PasqualiniD, BeruttiE.Isfractureresistanceofendodonticallytreated mandibularmolarsrestoredwithindirectonlaycomposite restorationsinfluencedbyfibrepostinsertion?JDent 2012;40(10):814–20,
http://dx.doi.org/10.1016/j.jdent.2012.06.005.
[34] VallittuPK.Impregnationofglassfibreswith
polymethylmethacrylatebyusingapowdercoatingmethod.
ApplComposMater1995;2:51–8.
[35] LeBellA-M,TannerJ,LassilaLVJ,KangasniemiI,VallittuPK.
Depthoflightinitiatedpolymerizationofglassfiber reinforcedcompositeinasimulatedrootcanal.IntJ Prosthodont2003;16:403–8.
[36] AromaaM,VallittuPK.Delayedpost-curingstageand oxygeninhibitionoffree-radicalpolymerizationof dimethacrylateresin.DentMater2018;34(9):
1247–52.
[37] ShahS,Shilpa-JainDP,VelmuruganN,SooriaprakasC, KrithikadattaJ.Performanceoffibrereinforcedcompositeas apost-endodonticrestorationondifferentendodontic cavitydesigns-anin-vitrostudy.JMechBehavBiomed Mater2020;104:103650,
http://dx.doi.org/10.1016/j.jmbbm.2020.103650.
[38] RobbinsJW.Restorationoftheendodonticallytreatedtooth.
DentClinNorthAm2002;46(2):367–84,
http://dx.doi.org/10.1016/s0011-8532(01)00006-4.
[39] WandscherVF,BergoliCD,LimbergerIF,ArdenghiTM, ValandroLF.Preliminaryresultsofthesurvivalandfracture loadofrootsrestoredwithintracanalposts:weakenedvs nonweakenedroots.OperDent2014;39(5):541–55, http://dx.doi.org/10.2341/12-465.
[40] FerrarioVF,SforzaC,SerraoG,DellaviaC,TartagliaGM.
Singletoothbiteforcesinhealthyyoungadults.JOral Rehabil2004;31(1):18–22,
http://dx.doi.org/10.1046/j.0305-182x.2003.01179.x.
[41] JantaratJ,PalamaraJE,MesserHH.Aninvestigationof cuspaldeformationanddelayedrecoveryafterocclusal loading.JDent2001;29(5):363–70,
http://dx.doi.org/10.1016/s0300-5712(01)00018-5.
[42] NishigawaK,BandoE,NakanoM.Quantitativestudyofbite forceduringsleepassociatedbruxism.JOralRehabil 2001;28(5):485–91,
http://dx.doi.org/10.1046/j.1365-2842.2001.00692.x.
[43] RahmanH,SinghS,ChandraA,ChandraR,TripathiS.
Evaluationoffractureresistanceofendodonticallytreated teethrestoredwithcompositeresinalongwithfibre insertionindifferentpositionsinvitro.AustEndodJ 2016;42(2):60–5,http://dx.doi.org/10.1111/aej.12127.
[44] BarbosaTdeS,MiyakodaLS,PocztarukRdeL,RochaCP, GaviãoMB.Temporomandibulardisordersandbruxismin childhoodandadolescence:reviewoftheliterature.IntJ PediatrOtorhinolaryngol2008;72(3):299–314,
http://dx.doi.org/10.1016/j.ijporl.2007.11.006.
[45] ZarowM,Ramírez-SebastiàA,PaoloneG,deRibotPortaJ, MoraJ,EsponaJ,etal.Anewclassificationsystemforthe restorationofrootfilledteeth.IntEndodJ2018;51(3):318–34, http://dx.doi.org/10.1111/iej.12847.
[46] Ami ˇzi ´cIP,Mileti ´cI,BarabaA,FanY,NathansonD.Invitro retentionofprefabricatedandindividuallyformedposts:a pilotstudy.JProsthetDent2018;120(4):553–7,
http://dx.doi.org/10.1016/j.prosdent.2018.04.011.
[47] DoshiP,KanaparthyA,KanaparthyR,ParikhDS.A ComparativeAnalysisofFractureResistanceandModeof FailureofEndodonticallyTreatedTeethRestoredUsing DifferentFiberPosts:AnInVitroStudy.JContempDentPract 2019;20(10):1195–9.
[48] FráterM,ForsterA,JantyikÁ,BraunitzerG,NagyK,Grandini S.Invitrofractureresistanceofpremolarteethrestored withfibre-reinforcedcompositepostsusingasingleora multi-posttechnique.AustEndodJ2017;43(1):16–22, http://dx.doi.org/10.1111/aej.12150.
[49] LeBell-RönnlöfAM,LassilaLV,KangasniemiI,VallittuPK.
Load-bearingcapacityofhumanincisorrestoredwith variousfiber-reinforcedcompositeposts.DentMater 2011;27(6),e107-115.doi:10.1016/j.dental.2011.02.009.
[50] VallittuPK.Arewemisusingfiberposts?Guesteditorial.
DentMater2016;32(2):125–6.
[51] BelliS,EraslanO,EskitasciogluG,KarbhariV.Monoblocksin rootcanals:afiniteelementalstressanalysisstudy.Int EndodJ2011;44(9):817–26.
[52] GaroushiS,GargoumA,VallittuPK,LassilaL.Short fiber-reinforcedcompositerestorations:areviewofthe currentliterature.JInvestigClinDent2018;9(3),e12330.doi:
10.1111/jicd.12330.
[53] Bijelic-DonovaJ,GaroushiS,LassilaLV,KeulemansF,Vallittu PK.Mechanicalandstructuralcharacterizationof
discontinuousfiber-reinforceddentalresincomposite.J Dent2016;52:70–8,
http://dx.doi.org/10.1016/j.jdent.2016.07.009.
[54] VallittuPK.Highaspectratiofillers:fiber-reinforced compositesandtheiranisotropicproperties.DentMater 2014;31:1–7.
[55] LassilaL,KeulemansF,SäilynojaE,VallittuPK,GaroushiS.
Mechanicalpropertiesandfracturebehaviorofflowable fiberreinforcedcompositerestorations.DentMater 2018;34(4):598–606,
http://dx.doi.org/10.1016/j.dental.2018.01.002.
[56] LassilaL,SäilynojaE,PrinssiR,VallittuP,GaroushiS.
Bilayeredcompositerestoration:theeffectoflayerthickness onfracturebehavior.BiomaterInvestigDent2020,inpress.
[57] GaroushiS,LassilaLV,TezvergilA,VallittuPK.Staticand fatiguecompressiontestforparticulatefillercomposite resinwithfiber-reinforcedcompositesubstructure.Dent Mater2007;23(1):17–23,
http://dx.doi.org/10.1016/j.dental.2005.11.041.
[58] OmranTA,GaroushiS,LassilaLV,VallittuPK.Effectof interfacesurfacedesignonthefracturebehaviorof bilayeredcomposites.EurJOralSci2019;127(3):276–84, http://dx.doi.org/10.1111/eos.12617.
[59] KrejciI,DucO,DietschiD,deCamposE.Marginal adaptation,retentionandfractureresistanceofadhesive compositerestorationsondevitalteethwithandwithout posts.OperDent2003;28(2):127–35.
[60] FokkingaWA,LeBellAM,KreulenCM,LassilaLV,VallittuPK, CreugersNH.Exvivofractureresistanceofdirectresin compositecompletecrownswithandwithoutpostson maxillarypremolars.IntEndodJ2005;38(4):230–7, http://dx.doi.org/10.1111/j.1365-2591.2005.00941.x.
[61] SisoSH,HürmüzlüF,TurgutM,Altundas¸arE,SerperA,ErK.
Fractureresistanceofthebuccalcuspsofrootfilled maxillarypremolarteethrestoredwithvarioustechniques.
IntEndodJ2007;40(3):161–8,
http://dx.doi.org/10.1111/j.1365-2591.2007.01192.x.
[62] NamSH,ChangHS,MinKS,LeeY,ChoHW,BaeJM.Effectof thenumberofresidualwallsonfractureresistances,failure patterns,andphotoelasticityofsimulatedpremolars restoredwithorwithoutfiber-reinforcedcompositeposts.J Endod2010;36(2):297–301,
http://dx.doi.org/10.1016/j.joen.2009.10.010.
[63] ScottiN,EruliC,CombaA,PaolinoDS,AlovisiM,Pasqualini D,etal.Longevityofclass2directrestorationsinroot-filled teeth:aretrospectiveclinicalstudy.JDent
2015;43(5):499–505,
http://dx.doi.org/10.1016/j.jdent.2015.02.006.
Pleasecitethisarticleinpressas:FráterM,etal.Fatiguebehaviorofendodonticallytreatedpremolarsrestoredwithdifferentfiber-reinforced [64] Tezvergil-MutluayA,VallittuPK.Effectsoffiber-reinforced
compositebasesonmicroleakageofcompositerestorations inproximallocations.OpenDent2014;8:213–9.
[65] LiX,PongprueksaP,VanMeerbeekB,DeMunckJ.Curing profileofbulk-fillresin-basedcomposites.JDent 2015;43(6):664–72,
http://dx.doi.org/10.1016/j.jdent.2015.01.002.
[66] LehtinenJ,LaurilaT,LassilaLVJ,TuusaS,KienanenP,Vallittu PK,etal.Opticalcharacterizationof
bisphenol-A-glycidyldimethacrylate-triethylene glycoldimethacryalatemonomersandcopolymers.Dent Mater2008;24:1324–8.