Current Physical Status Evaluation Subsystem using User-specific tuned Membership Functions
in Sport Activity Risk Calculation
Edit Tóth-Laufer*, Márta Takács**, Zoltán Keresztényi***,
* Óbuda University/Doctoral School of Applied Informatics, Budapest, Hungary
** Óbuda University/John von Neumann Faculty of Informatics, Budapest, Hungary
*** Oxygen Medical, Budapest, Hungary
laufer.edit@bgk.uni-obuda.hu, takacs.marta@nik.uni-obuda.hu, keresztenyi@gmail.com
Abstract—In this paper a subsystem of a fuzzy logic-based sport activity risk level calculation model is presented. This subsystem evaluates the risk from the patient’s measured physiological parameters as heart rate, systolic and diastolic blood pressure in real-time. For the most reliable results the input membership functions are tuned according to the influential parameters on the measured factors before the real time calculation offline. The obtained membership functions are user-specific thus the result of the evaluation is more reliable.
I. INTRODUCTION
Health promoting effects and rehabilitation role of sport is clear to everyone. Sport has an important role in active lifestyle and it improves the quality of life. These statements are only true if the personal capability and medical recommendations are taken into account.
Otherwise it can be dangerous due to the harmful or overdriven activity. The chronic diseases, actual physical condition, age, and many other sub-factors should be considered, in order to keep the practiced sport to be safe and healthy rather than becoming the situation worse. The author’s model calculates the risk level of sport activity from personal parameters, among them some real-time measured parameters as heart rate, systolic and diastolic blood pressure.
There is no clear agreement about the abnormal blood pressure response during progressive tests and the parameters and methods are different in the studies, but it is obvious that the commonly used absolute values are useless. Patient-specific thresholds should be given taking into account several personal parameters as the patient’s age, sex, resting systolic blood pressure and the health state of the patient or the target of the sport activity. Using these influential parameters the membership functions can be tuned, which is essential for proper risk level calculation. In this way can be avoid that case, when the same blood pressure value of a 25-year-old and a 70-year- old patient is evaluated as the same risk level. Another example when patients in different health state are compared. In this case the meaning of the same heart rate value is different for a patient who works out and practices athletics regularly or a patient who is under rehabilitation [1].
The thresholds cannot be defined as exact values; the boundaries between the normal and increased or abnormal response are vague so that can be handled by the fuzzy
approach. Fuzzy logic-based decision making in risk management is also very advantageous, because it can handle the uncertainty, imprecision and subjectivity in the data and in the evaluation process [2].
This paper focuses on a subsystem of the authors’ sport activity risk level calculation model, namely the “Current physical status” subsystem, because this is the group where the user-specific tuned membership functions are the most needed. It measures several physiological parameters of the patient in real-time. These parameters are the heart rate, systolic and diastolic blood pressure, which are evaluated to calculate the actual risk level.
These input parameters are the most common ones in similar monitoring systems, but among the measured physiological parameters can be the blood oxygen saturation level (SpO2), electrocardiograph (ECG), electroencephalography (EEG), perspiration, respiration rate, body surface temperature and weight [3],[4].
In order for the membership functions belonging to the above mentioned physiological parameters, to be properly tuned, some additional personal parameters (age, sex, target of the training) are also necessary. The task of the system is to send an alert to the patient itself or to other specified persons if the risk level is too high. The alert must be sent in time to avoid the serious consequences, therefore the evaluation time should not be too long. In the monitoring systems the alarm usually sent via cellular phone [3], or over the Internet, even multiple recipients [5]. The message can be obtained the global position system (GPS) to indentify the location and the abnormal values, which caused the alarm [6]. Reducing the computational complexity also reduces the time factor, thus the rule base and evaluation structure reduction is necessary. Some of potential methods used by the authors are also presented in the paper.
II. THE MODEL STRUCTURE
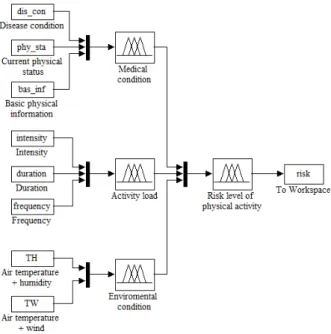
The authors’ model has a hierarchical multilevel structure, which is simplifies the evaluation and can be easily expanded. The evaluation is fuzzy logic-based with Mamdani-type inference system. The structure of the model follows the logic of the evaluation. On the left side there are the input factors whose evaluation are done in groups at the next higher level and the result is transmitted to the highest level where the overall risk level is calculated. The grouping is based on the input characteristics. The first group describes the patient’s
medical condition including the chronic diseases (“Disease condition”), the patient’s age, sex and occupation (“Basic physical information”) and the actual condition (“Current physical status”). This main group is called “Medical condition”. The second main group
“Activity load” is used for the characterization of the sport activity itself. These parameters describe how intensively, how long per occasion and how many times per week the patient does this activity. The last group “Environmental condition” summarizes the influence of the environmental factors with combined input parameters. In these inputs the air temperature is combined with such parameters which also have an influence on thermal sensation. These combined factors are air temperature and humidity together (TH), as well as air temperature and wind together (TW). The structure of the model is shown in Fig.
1.
There are several input factors, which do not change during the monitoring and some groups have only these kinds of inputs. For these subsystems the evaluation can be performed offline before the monitoring, thereby they do not affect the computational complexity of the real- time evaluation. The parameters of the other groups such as “Current physical status” subsystem, which is the main topic of this paper, change in real-time therefore there is a need to reduce the computational complexity. The possible reduction techniques used by the authors are presented in Section V.
Figure 1. The fuzzy model structure III. THE STRUCTURE OF THE SUBSYSTEM A. The input data
The “Current physical status” subsystem evaluates the real-time risk level of the monitored patient’s sport activity based on several measured parameters. These parameters are the heart rate (HR), systolic blood pressure (SBP) and diastolic blood pressure (DBP). If the heart rate or the systolic blood pressure is taken into account the number of these influential factors are about thirty. The most common ones among them are age, sex, weight, time of day, air temperature, humidity, physical fitness, intensity of activity, mood, drugs and certain diseases [7].
In order to define user-specific membership functions the influential factors are also necessary as input parameters.
It is very difficult to see through the combined effect the large number of these factors even for the experts, therefore only the fundamental factors was taken into consideration. To determine the membership functions of the heart rate, the first of these input parameters is the maximum heart rate, which is the highest value that can be achieved at physical limit load. The exact patient-specific value can be obtained as a result of progressive exercise testing, but it can be performed only in laboratory and for some groups of the patients with chronic diseases not at all. To avoid the above problems and the physical load risk, the authors used the much safer predictive maximum heart rate during the evaluation. There are several methods to determine this estimated or calculated value. The most popular among them is the age-based one due to its simplicity. It calculates the maximum heart rate with the equation “220-age”, but it does not take into account the patient’s other characteristics thereby it can be significantly different from the actual value. An important consideration is when selecting the method that the maximum heart rate is not a constant value even for the same patient it may vary depending on the circumstances.
For these reasons the predicted maximum heart rate (HRmax-p) calculated by Polar RS800CX run training computer is used in the model. The measurement method of the device allows ECG accurate heart rate detection and takes into account the personal parameters and current circumstances during the calculation. The maximum heart rate can be obtained in this way with an approximately five-minute test before the monitoring. To tune the membership functions of the actual heart rate and blood pressure properly the target of the training is also need to be known. The target zones used by the authors are based on the Polar heart-rate zones [8], but the focus was on risk calculation instead of the effectiveness of the training, accordingly the zones are modified. These modified target zones proposed by the authors are shown in Table I. The basis of the appropriate zone selection can also be the medical recommendations based on the patient’s health state or physical fitness.
In the literature particularly the resting blood pressure data can be found, there are relatively few studies about the effect of the stress test on blood pressure and even today there is no clear consensus on where the threshold of abnormal blood pressure response is. The parameters and methods in these studies are different, but the most commonly used one is the absolute figure, due to its simplicity. Nevertheless it determines the threshold regardless of the patient’s age, sex, health state and other influential parameters. This approach can cause relatively
TABLE I. TARGET ZONES
Intensity % of HRmax
(bpm) Recommended for
<50% Medical treatment, rehabilitation, cardiac disease
50-70% Prevention, beginner, basic training
70-95% Athletes regularly
large errors in risk level calculation, because the same systolic blood pressure values do not have the same clinical significance for a younger or an older patient; or the same age patients, whose health state are different.
The other commonly used approach considered the patient’s age and sex to determine the thresholds, but physical fitness of the patient is also ignored by them. The basis of the appropriate blood pressure membership function determination is the method proposed by Sieira et al. [1]. In addition the age and sex of the patient they take into account also the physical fitness by a calculated value, which is the so-called deltaSPB. DeltaSPB can be calculated as SBPmax-SBPrest and this value implies that the fitter the patient, the higher this value [1]. This approach was modified by the authors such that the target zones are also included the systolic blood pressure threshold calculation thereby the medical recommendations can be also taken into account. The diastolic blood pressure stagnates or decreases during the activity.
The structure of the Current physical status subsystem is shown in Fig. 2. where the input factors are on the left side and the influential factors, which are necessary to tune the membership functions are the top of the figure.
The input factors are the heart rate (HR), the systolic blood pressure (SBP) and the diastolic blood pressure (DBP), the influential factors are the maximum heart rate (HRmax), the resting systolic blood pressure (SBPrest), age, sex and the target of the training. This subsystem is the details of the “Current physical status” input in the overall model, whose structure is shown in Fig. 1.
Figure 2. The Current physical status subsystem B. The patient-specific tuned membership functions
Using the above-described influential parameters the membership functions can be tuned according to the patient characteristics. To define the membership functions of the heart rate, the predicted maximum heart rate and the recommended intensity (Table I.) should be considered. There are three antecedent fuzzy sets: “target”
is the ideal heart rate zone for the patient, “mhigh” is an increased heart rate and “vhigh” is very high, which is not allowed for the patient. The zones and the actual input value are defined as a percentage of the maximum heart rate of the person. The heart rate antecedent sets of a patient who is under rehabilitation can be seen in Fig. 3.
and for a beginner patient are shown in Fig. 4.
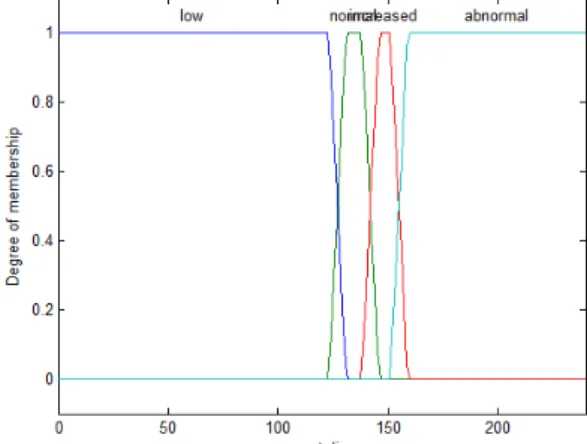
The systolic blood pressure membership functions are defined as a combination of the values specified by Sieira et al. (Table II.) and the thresholds calculated by (1) and (2). The antecedent fuzzy sets are “low” which represents the hypotonic values, “normal” is the desired SBP value,
“increased” is a somewhat higher value as desired but acceptable and “abnormal” is not recommended for the patient due to the higher risk. The name of the diastolic
blood pressure antecedent sets are the same as the systolic blood pressure antecedent sets, but the limits are obviously different from that.
Figure 3. Heart rate antecedent sets for a patient under rehabilitation
Figure 4. Heart rate antecedent sets for beginner patient
( ) (
minnormal rest)
restmin target SBP SBP *target SBP
SBP = − + (1)
( ) (
maxnormal rest)
restmax target SBP SBP *target SBP
SBP = − + (2)
where target is the center of the target zone,
SBP
maxnormaland
SBP
minnormalare the threshold values in the method of Sieira et al. [1], SBPrest is the resting heart rate of the patient. The systolic blood pressure antecedent sets for aTABLE II. NORMAL BLOOD PRESSURE RESPONSE
Age Men Women
Systolic Diastolic Systolic Diastolic 20-29 161-203 59-83 136-176 58-82 30-39 164-204 64-88 138-182 63-85 40-49 167-209 68-92 144-190 67-89 50-59 170-216 71-95 153-201 69-93 60-69 173-221 72-96 162-210 68-84 70-79 169-223 71-97 160-210 73-93
35-year-old woman, who is under rehabilitation, are shown in Fig. 5. and for a same age beginner woman are depicted in Fig. 6.
Figure 5. Systolic blood pressure antecedent sets for a 35-year-old woman under rehabilitation
Figure 6. Systolic blood pressure antecedent sets for a 35-year-old beginner woman
IV. TEST RESULTS
The input parameters during the verifying test were theoretical. The parameter selection covers the values of healthy patients of both sexes for all ages and all target zones as it is described in Section III. The goal was to validate the real-time subsystem with tuned antecedent membership functions. The test was performed 576 different cases by varying the input parameters and the results were verified by an expert. Selection of the parameters was designed to cover the most possible cases.
Some examples are presented in the following. The input parameters - systolic blood pressure (SBP), the diastolic blood pressure (DBP), the current heart rate (HR), the maximum heart rate (HRmax), the target of the training (target) based on Table I, the age and sex of the patient - are shown in Table III, for sake of simplicity the resting heart rate is set to 70 bpm and the resting systolic blood pressure is 120 mmHg. The calculated SBP limits based on these values are presented in Table IV, where the thresholds of the SBP ranges are defined. These ranges are low, when the value is lower than it is fit; normal is the appropriate range, increased is slightly higher than the corresponding value and abnormal is excessive SBP
response. The four input membership functions’
parameters belong to these limits can be seen in Table V.
and VI. Last but not least the calculated risk levels are shown in Table VII.
TABLE VI. MEMBERSHIP FUNCTION PARAMETERS
increased abnormal a b c d a b
186.54 197.19 202.51 213.16 202.51 213.16 192.54 204.14 209.95 221.55 209.95 221.55 165.25 186.54 197.19 218.48 197.19 218.48 169.33 192.54 204.14 227.36 204.14 227.36 186.54 197.19 202.51 213.16 202.51 213.16 165.25 186.54 197.19 218.48 197.19 218.48
TABLE III. INPUT PARAMETERS
SBP DBP HR HRmax target age sex 175 80 107 165 50-70% 50-59 male 160 99 124 165 70-85% 50-59 male 145 70 91 165 50-70% 50-59 fem.
155 105 124 165 70-85% 50-59 fem.
170 70 91 185 50-70% 30-39 male 190 80 107 185 50-70% 30-39 fem.
TABLE V. MEMBERSHIP FUNCTION PARAMETERS
low normal a b a b c d 154.6 165.25 154.6 165.25 186.54 197.19 157.7 169.33 157.7 169.33 192.54 204.14 135.7 157.00 135.7 157.00 165.25 186.54 137.1 160.33 137.1 160.33 169.33 192.54 149.8 160.46 149.8 160.46 186.54 197.19 125.3 146.62 125.3 146.62 165.25 186.54
TABLE IV. LIMITS
Low max
Normal min
Normal max
Increased min
Increased max
Abnormal min 159.9 159.9 191.86 191.86 207.83 207.83 163.5 163.5 198.34 198.34 215.75 215.75 146.4 146.4 175.89 175.89 207.83 207.83 148.7 148.7 180.93 180.93 215.75 215.75 155.1 155.1 191.86 191.86 207.83 207.83 135.9 135.9 175.89 175.89 207.83 207.83
V. POSSIBLE WAYS TO REDUCE THE COMPUTATIONAL COMPLEXITY IN THE SYSTEM
In this risk calculation model there are some groups which parameters should be evaluated in real-time. In these kinds of systems to minimize the computational complexity and time are essential to conceive the decision in time. Therefore the complexity reduction methods in rule base and in the evaluation structure are of key importance. Primarily the exact reduction is desired, but in some cases a non-exact reduction can be allowed if the circumstances justify it and in this way a serious consequence can be prevent. These methods should be used for all of the subsystems that take part of the real- time calculation. In this section the possible methods used by the authors are presented. The membership function tuning can be used simultaneously with the rule interconnection or the HOSVD-based rule base reduction.
A. Membership function tuning as preprocessing
In the literature there are many adaptive fuzzy applications where the number of the rules is fixed and the membership functions are tuned. They are used particularly in non-linear systems with unknown dynamic models [9]. Another possibility is operating for the evolutionary optimization algorithms, where an objective function is used [10],[11].
In the above described system some of the parameters, which are used as a basis of the tuning the membership functions are constant and the others quasi-constant, i.e.
do not change during the test, maybe for the following test day. Therefore the tuning can be performed before the evaluation as an off-line preprocessing part of the system.
The method can be based on the above described calculated thresholds or the aggregated input membership functions suggested by the authors in [12]. The latter method is able to handle the complex interactions between the input factors by regressing them to simpler and manageable ones. In this case the known effects are described separately by membership functions and their combined effect is obtained after their aggregation [12].
B. Interconnection of the rules
The authors’ risk calculation model uses a multiple rule base due to the hierarchical structure if the overall model structure is considered, i.e. the inputs are mapped to the outputs taking the intermediate variables into account. The rule interconnection is performed in the subsystems separately, where single rule base is used, i.e. the inputs are mapped directly to the outputs [13]. In these kinds of systems the rule consequents can be the same in different rules. Taking advantage of this system characteristic,
those rule antecedents which have the same consequent part can be connected together with a disjunction operator.
The authors found that using the maximum and probor operators for the interconnection does not change the result of the evaluation [14]. This simplification can be made in the fuzzy and neuro-fuzzy model as well and it improves the model efficiency. In the literature there is a relatively novel type of fuzzy system, called fuzzy network where the mapping from the inputs to the outputs is similar to the multiple rule base system, but each subsystem has a node belonging to it and the interaction between the subsystems is represented by the connection of these nodes. It can be modeled by a fuzzy network grid and interconnection structure, which specifies only the location of the nodes and the connection between them, thus it is a useful tool for formal modeling of the fuzzy network with a higher level of abstraction. The rule interconnection used by the authors is similar to the vertical merging of nodes in the fuzzy network, where the parallel nodes are merged [13],[15].
C. HOSVD-based rule base reduction
The Higher Order Singular Value Decomposition (HOSVD) method reduces the complexity of the rule base in an exact or non-exact way. The exact reduction means that in the system there is a redundancy and only this is filtered out from the system. The other feature is the non- exact reduction when the weakly contributing parts are filtered out, based on an error estimation. In this system the latter can be used with calculating the acceptable error level and it is used as a threshold value of the reduction [15],[16]. In practical cases the approximation never achieves the zero error, i.e. it has no universal approximation property [17]. This approach is useful in unexpected situations when the decision must be made in a short time, because any delay could have serious consequences. In this case a slight error, that does not affect the decision-making, is allowed if this reduction makes the evaluation faster [16],[18]. A disadvantage of this approach is that the reduced rule base adaptation to the new information raises problems, if the new information cannot be described by the rules of the reduced rule base. In these cases new rules should be added to the reduced rule base, or the antecedent sets of the reduced rule base should be modified to describe the new information, which one is preferred from the system’s point of view [17]. The HOSVD method can also be used in tensor product dynamic models, which is a field of intelligent systems, and it is used in strongly non-linear system approximation [19] and for LPV model reduction and multidimensional data representation [20].
VI. CONCLUSIONS
In risk level calculation of sport activity the real-time evaluation is indispensable. Several values should be monitored in real-time during the evaluation and there are several factors, which have an influence on them. These influential factors must be also taken into consideration.
There is a need to tune the membership functions to obtain patient-specific fuzzy sets and in this way the calculated risk level is more reliable. The authors implemented a real-time subsystem, which is able to tune the antecedent membership functions based on the influential parameters of the measured values. This subsystem is verified by an expert and it proved to be reliable. The tuning can be TABLE VII. RISK LEVEL
Numerical Liguistic
0.1625 Very safe
0.5000 Medium 0.2607 Moderately safe 0.8499 Very dangerous
0.1625 Very safe
0.2754 Moderately safe
performed off-line before the monitoring, thus it does not increase the computational complexity of the real-time evaluation. There are some other complexity reduction techniques proposed by the authors, as the interconnection of the rules and HOSVD-based rule base reduction. These techniques ensure that the alert is sent in time preventing the serious consequences.
ACKNOWLEDGMENT
The authors gratefully acknowledge the grant provided by the project TÁMOP-4.2.2/B-10/1-2010-0020, Support of the scientific training, workshops, and establish talent management system at Óbuda University and the Hungarian Scientific Research Fund (OTKA K 105846).
REFERENCES
[1] M. C. Sieira, A. O. Ricart, R. S. Estrani, “Blood pressure response to exercise testing“ in Apunts Med Esport., Elsevier, 2010, pp.
191-200.
[2] M. Takács, Multilevel Fuzzy Approach to the Risk and Disaster Management, Acta Polytechnica Hungarica, Vol. 7, Issue No.4, (2010).
[3] J. Min Kang, T. Yoo, H.Chan Kim, “A Wrist-Worn Integrated Health Monitoring Instrument with Tele-Reporting Device for Telemedicine and Telecare”, IEEE Transactions on Instrumentation and Measurement, Vol. 55, No. 5, October 2006, pp. 1655-1661, doi: 10.1109/TIM.2006.881035.
[4] F. Rahnman, A. Kumar, G. Nagendra, G. Sen Gupta, “Network Approach for Physiological Parameters Measurement”, IEEE Transactions on Instrumentation and Measurement, Vol. 54, No. 1, February 2005, pp. 337-346., doi: 10.1109/TIM.2004.834595 [5] F. Rahnman, A. Kumar, G. Nagendra, G. Sen Gupta, “Network
Approach for Physiological Parameters Measurement”, IEEE Transactions on Instrumentation and Measurement, Vol. 54, No. 1, February 2005, pp. 337-346., doi: 10.1109/TIM.2004.834595 [6] L. Fanucci, S. Saponara, T. Bacchillone, M. Donati, P. Barba, I.
Sánchez-Tato, C. Carmona, “Sensing Devices and Sensor Signal Processing for Remote Monitoring of Vital Signs in CHF Patients”, IEEE Transactions on Instrumentation and Measurement, Vol. 65, No. 3, March 2013, pp. 553-569, doi:
10.1109/TIM.2012.2218681
[7] E. Dömötör, “Pulzuskontroll, testsúlykontroll”, Carita Bt, 2005, ISBN: 963-86741-0-5.
[8] Polar RS100 User Manual, http://www.polarusa.com/support_files /us-en/85256F470048B0BC852574730060F559/Polar_RS100_
user_manual_English.pdf
[9] M. Moradi, M. H. Kazemi, and E. Ershadi, "Direct adaptive fuzzy control with membership function tuning," Asian J. Control, vol.
14, pp. 726–735, May 2012.
[10] R.-E. Precup, R.-C. David, E. M. Petriu, M.-B. Radac, S. Preitl, and J. Fodor, "Evolutionary optimization-based tuning of low-cost fuzzy controllers for servo systems," Knowl.-Based Syst., vol. 38, pp. 74-84, Jan. 2013.
[11] S. Szénási, Z. Vámossy, M. Kozlovszky, “Preparing Initial Population of Genetic Algorithm for Region Growing Parameter Optimization”, 4th IEEE International Symposium on Logistics and Industrial Informatics (LINDI), 5-7. Sept, 2012, pp. 47-54.
[12] E. Tóth-Laufer, M. Takács, I. J. Rudas, "Interactions Handling Between the Input Factors in Risk Level Calculation" in IEEE 11th International Symposium on Applied Machine Intelligence and Informatics (SAMI 2013), Herl'any, Slovakia, January 31- February 2, 2013, pp. 71-76, ISBN: 978-1-4673-5926-9, IEEE catalog number: CFP1308E-PRT, DOI: 10.1109/SAMI.2013.
6480947.
[13] A. Gegov, Fuzzy Networks for Complex Systems - A Modular Rule Base Approach. Berlin, Heidelberg: Springer-Verlag, 2010.
[14] E. Tóth-Laufer, M. Takács, I.J. Rudas, "Conjunction and Disjunction Operators in Neuro-Fuzzy Risk Calculation Model Simplification" in 13th IEEE Internation Symposium on Computational Intelligence and Informatics (CINTI 2012), Budapest, Hungary, November 20-22, 2012, pp. 195-200, ISBN:
978-1-4673-5204-8, IEEE Catalog Number: CFP1224M-PRT, DOI: 10.1109/CINTI.2012.6496759 .
[15] A. Gegov, "Advances in fuzzy systems and networks," in Proc.
IEEE Conf. of Intelligent Systems (IS 2012), Sofia, Bulgaria, 2012, pp. 33-40.
[16] A.R. Várkonyi-Kóczy, “Model Based Anytime Soft Computing Approaches in Engineering Applications.” In Balas, V., J. Fodor, A.R. Várkonyi-Kóczy (eds.), Soft Computing Based Modeling in Intelligent Systems (Ser. Studies in Computational Intelligence), Springer Verlag, Berlin, Heidelberg, 2009, pp. 63-92.
[17] P. Baranyi, A. R. Varkonyi-Koczy, Y. Yamm, and R. J. Patton,
"Adaptation of TS fuzzy models without complexity expansion:
HOSVD-based approach," IEEE Trans. Instrum. Meas., vol. 54, No.1, pp. 52-60, Feb. 2005.
[18] E. Tóth-Laufer, A.R. Várkonyi-Kóczy, "Anytime Sport Activity Risk Level Calculation using HOSVD based Hierarchical Fuzzy Models" in IEEE International Symposium on Medical Measurements and Applications (MeMeA), Gatineau, Quebec, Canada, May 4-5, 2013
[19] P. Baranyi, L. Szeidl, P. Várlaki, and Y. Yam, "Definition of the HOSVD-based canonical form of polytopic dynamic models," in Proc. 3rd International Conference on Mechatronics (ICM 2006), Budapest, Hungary, 2006, pp. 660-665.
[20] A. Rövid, L. Szeidl, P. Várlaki “HOSVD Based Data Representation and LPV Model Complexity Reduction”, Applications of Mathematics and Computer Engineering - American Conference on Applied Mathematics, AMERICAN- MATH'11, 5th WSEAS International Conference on Computer Engineering and Applications, CEA'11, Mexico, January 29-31, 2011, pp. 164-169.