Distal versus conventional radial access for coronary angiography and intervention:
Design and rationale of DISCO RADIAL study ✩
AdelAminian,MDa,GregoryA.Sgueglia,MDPhDb,MarcusWiemer,MDc,GabrieleLuigiGasparini,MDd, JoelleKefer,MDPhDe,ZoltanRuzsa,MDPhDf,g,MaartenA.H.vanLeeuwen,MDPhDh,BertVandeloo,MDi, ClaudiuUngureanu,MDj,SaskoKedev,MDPhDk,JuanFIglesias,MDPhDl,GregorLeibundgut,MDm, KarimRatib,MBChBn,IvoBernat,MDPhDo,IreneBarriocanal,MScp,VladimirBorovicanin,MDp,and ShigeruSaito,MDPhDqSzeged
Background
Transradialaccess(TRA)hasbecomethedefaultaccessmethodforcoronarydiagnosticandinterven- tionalprocedures.Ascomparedtotransfemoralaccess, TRAhasbeenshowntobesafer,cost-effectiveandmore patient- friendly. Radial artery occlusion (RAO)represents the most frequentcomplication of TRA, andprecludes futurecoronary proceduresthroughtheradialartery,theuseoftheradialarteryasaconduitforcoronaryarterybypassgraftingorasar- teriovenousfistulaforpatientsonhemodialysis.Recently,distalradialaccess(DRA)hasemergedasapromisingalternative toTRA, yieldingpotential forminimizingthe riskofRAO. However, aninternationalmulticenter randomizedcomparison betweenDRA,andconventionalTRAwithrespecttotherateofRAOisstilllacking.Trial Design
DISCO RADIAL is a prospective, multicenter, open-label,randomized, controlled, superioritytrial. A totalof1300eligiblepatientswillberandomlyallocatedtoundergocoronaryangiographyand/orpercutaneouscoronary intervention(PCI)throughDRAorTRAusingthe6FrGlidesheathSlendersheathintroducer.Extendedexperiencewithboth TRAandDRAisrequiredforoperators’eligibilityandoptimalevidence-basedbestpracticetoreduceRAO systematically implementedbyprotocol.TheprimaryendpointistheincidenceofforearmRAOassessedbyvascularultrasoundatdischarge.Severalimportantsecondaryendpointswillalsobeassessed,includingaccess-sitecross-over,hemostasistime,andaccess-site relatedcomplications.
Summary
TheDISCORADIALtrialwillprovidethefirstlarge-scalemulticenterrandomizedevidencecomparingDRA toTRAinpatientsscheduledforcoronaryangiographyorPCIwithrespecttotheincidenceofRAOatdischarge.(AmHeart J2022;244:19–30.)Keywords:Distalradialaccess;Radialarteryocclusion;Transradialaccess;Transradialapproach
FromtheaDepartmentof Cardiology,CentreHospitalierUniversitairedeCharleroi, Charleroi, Belgium,bDivision of Cardiology, Sant’Eugenio Hospital, Rome, Italy, cDepartmentofCardiologyandIntensiveCare,JohannesWeslingUniversityHospital RuhrUniversityBochum,Minden,Germany,dHumanitasClinicalandResearchCenter, IRCCS,Rozzano-Milan,Italy,eDivisionofCardiology,CliniquesUniversitairesSaint-Luc, Brussels,Belgium,fDepartmentofInternalMedicine,InvasiveCardiologyDivision,Uni- versityofSzeged,MedicalFaculty,Szeged,Hungary,gCardiologyDivision,Bács-Kiskun CountyHospital,InvasiveCardiology,Kecskemét,Hungary,hDepartmentofCardiology, IsalaHeartCenter,Zwolle,theNetherlands,iDepartmentofCardiology,Universitair ZiekenhuisBrussel,VrijeUniversiteitBrussel(VUB),Brussels,Belgium,jDepartmentofCar- diology,JolimontHospital,LaLouvière,Belgium,kInterventionalCardiologyDepartment, UniversityClinicofCardiology,Skopje,Macedonia,lDepartmentofCardiology,Geneva UniversityHospital,Geneva,Switzerland,mKantonsspitalBaselland,Liestal,Switzer- land,nCentreforPrognosisResearch,KeeleCardiovascularResearchGroup,Institutefor PrimaryCareandHealthSciences,KeeleUniversity,UnitedKingdom,oDepartmentof Cardiology,UniversityHospitalandFacultyofMedicinePilsen,CharlesUniversity,Pilsen, CzechRepublic,pEuropeanMedicalandClinicalDivision,TerumoEuropeN.V.,Leuven, Belgium,qDepartmentofCardiology,ShonanKamakuraGeneralHospital,Kanagawa, Japan
Abbreviations:ACS,Acutecoronarysyndrome;DRA,Distalradialaccess;EACTS,Euro- peanAssociationforCardio-ThoracicSurgery;EAPCI,EuropeanAssociationofPercuta-
Transradialaccess(TRA)hasbecomethestandardvas- cularaccessforcoronaryangiographyandpercutaneous coronary intervention (PCI) and is currently endorsed withaclassIA recommendationinthelatestEuropean
neousCardiovascularInterventions;ESC,EuropeanSocietyofCardiology;Fr,French;ITT, Intention-to-treat;PCI,Percutaneouscoronaryintervention;PP,Perprotocol;RAO,Radial arteryocclusion;TFA,Transfemoralaccess;TRA,Transradialaccess.
$AdelAminianandGregoryA.Sguegliacontributedequallytothisworkandarejoint firstauthors.
SubmittedJuly30,2021;acceptedOctober2,2021
Reprintrequests:AdelAminian,MD,DepartmentofCardiology,CentreHospitalierUni- versitairedeCharleroi,Charleroi,Belgium
E-mailaddress:adaminian@hotmail.com. 0002-8703
© 2021 The Author(s). Published by Elsevier Inc.
This is an open access article under the CC BY license (http://creativecommons.org/licenses/by/4.0/)
https://doi.org/10.1016/j.ahj.2021.10.180
Society of Cardiology/European Associationfor Cardio- ThoracicSurgery(ESC/EACTS)Guidelinesonmyocardial revascularization,irrespectiveofclinicalpresentation.1-3 Similarly,aradialfirststrategyinpatientswithacutecoro- narysyndromes(ACS)hasbeenadvocatedinaScientific StatementfromtheAmericanHeartAssociation.4
Multiplestudiesandmeta-analysiscomparingTRAver- sus transfemoralaccess (TFA)have demonstratedcom- pellingevidenceforTRAtoreducetheriskforaccess-site bleedingandvascularcomplications,5-8 tobemorecost- effectivedue to a shorterhospital stay,9 , 10 to bemore patient friendly9 andto reduceall-causemortality.6 , 7 , 11 Thelatterisespeciallyevidentinhigh-riskpatientssuch asthosepresentingwithACS.5-7 , 11 Owingto suchrele- vantadvantages,TRAisalso increasinglyadoptedinan expandingrangeofnon–coronaryprocedures,including interventionaloncology,neuroradiology,andperipheral arterialinterventions.12
TheclinicalbenefitsofTRAhoweverrelyontheopera- tor’sexperienceandTRAmaybelimitedbyasmallerar- terialdiametercomparedtoTFAyieldingahigheraccess failurerate,vascularspasm, andradial arteryocclusion (RAO),acomplexprocessinvolvingseveralinterplaying factorsultimatelyleadingtothrombosis,withareported incidenceupto33%ofthecases.13 , 14 Owingtotheex- tensivenetworkofforearm vascularanastomoses,RAO is mostly asymptomatic, from an ischemia standpoint, yetitprecludestheuseofthesameradialarteryforfu- turepercutaneousdiagnostic,andinterventionalproce- dures.15 Suchacomplicationisexpectedtobeofgrow- ingimportancegiventhearrayoftransradialprocedures to whichthesameindividual maybe subjectedduring hislifetime.Moreover,anoccludedradialarteryisobvi- ouslynotsuitableasaconduitforcoronaryarterybypass graftingsurgeryorforanarteriovenousfistulainpatients requiringhemodialysis.
Several clinical and procedural characteristics have beenlinked totheoccurrenceofRAO,15 andbestprac- tices recommendations for the prevention of RAO in- clude reduction of the sheath/catheter size, adequate procedural anticoagulation, non–occlusive hemostasis, andaminimalpressurestrategywithshort(≤120min) hemostasistime.15-21 The useof thedistalradialartery, witharterialaccessintheanatomicalsnuffboxoronthe dorsumofthehand,hasrecentlyemergedasapromising alternativeaccessroutetofurtherreducetheriskofRAO, andhasbeenendorsedbyarecentInternationalConsen- susPaperonthepreventionofRAO.15 , 22 However,the levelofevidence insupportofthisrecommendation is limited.
Rationale fordistal radialaccess
Distallytothestyloidprocessoftheradiusbone,the radialarterygives riseto thesuperficial palmarbranch formingthesuperficialpalmararchandthencrossesthe
anatomicalsnuffboxbeneaththetendonsoftheabduc- torpollicislongusandtheextensorpollicisbrevismus- cles,justabovethescaphoid,andtrapeziumbones.The radialarterycontinues itscourseonthedorsumofthe handandfinallyswervesmediallyintothepalmtoform thedeep palmararchconnectingwith abranch ofthe ulnar artery.22 , 23 The distal radial artery may bepunc- turedproximallytothetendonof theextensor pollicis longusmuscleintheanatomicalsnuffboxordistallyto itinthedorsumofthehand(Figure1).These2alterna- tivepuncturepointsaredistaltothecarpalanastomotic networksand thesuperficial palmararchand yieldthe sameadvantagesasconventionalTRAwithanadditional potentialtomaintainantegradeflowintheforearmradial arteryduringhemostaticcompressionofthedistalradial artery,reducingtherebytheriskofretrogradethrombus formation,andforearmRAO.24
Theoccurrenceofthrombosisattheconventionalra- dialcannulationsitejustproximallytothestyloidprocess oftheradiusbonemayextendbackuptotheoriginof theradialarterythatgenerallylacksimportantbranching intheforearm.Contrariwise, ifthrombosiscomplicates avascularaccessintheanatomicalsnuffboxorthedor- sumofthehand,flowintheforearmradialarterywillbe maintained owingto thewrist and hand anastomoses, thuspreventingbloodstasisduringhemostasisandprox- imalthrombus growth.25 Thisdescription issupported bytheDistalRadial AccessDoppler Studythat demon- strated virtually unchanged flow in the forearm artery duringsimulatedRAO attheanatomical snuffboxlevel incontrasttotheseverereductionofflowobserveddur- ingsimulatedRAOatwrist.26
Moreover, thedistal radial arterylies in the subcuta- neousspace superficial to thefascial compartmentsof thehand,thusfavoringafaster,andsaferhemostasisas comparedtoconventionalTRA.Whenperformedinthe leftupper limb,anotherpotential advantage ofDRA is anergonomicallyimprovedpositionforboththeopera- torandthepatient,grantinganexcellentcompromiseto savetherightarmfromimmobilization.27
Thoserelevant advantagesarecontrastedbyaslightly smallersizeofthedistalradialarterypotentiallyimpact- ingondeviceselectionandproceduralplanningandby itslesspredictablecourse,duetothepronouncedtortu- osityandangulation ofthevessel, leadingtoanoverall highernumber of puncture attempts, a longer time to achievearterialaccess and a higher rateof access fail- ure.24
Criticalappraisal of theevidence
ThefeasibilityofDRAhasbeenevaluatedinanumber ofobservationalclinicalregistriesshowingsomevariabil- ityowingtotheinclusionincertainstudiesofthevery first DRA procedures performed by the operators.27-44 Yet, the overall success rate was high, and no major
Figure1
Anatomicallandmarkofdistalradialaccess.Violetarrowpointstoconventionaltransradialaccesspuncturesiteatwristlevel;turquoise arrowspointtothedistalradialaccesspuncturessitesintheanatomicalsnuffboxandinthedorsumofthehand.
safety signals have been reported despite the lack of specific attention paid to an optimal hemostasis. Espe- cially,therateofRAOwasextremelylowintheseearly series.
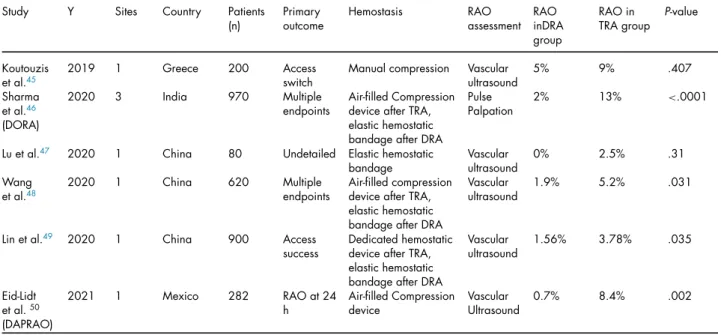
Moreover,a fewtrials havebeenperformed withthe aimto compareDRA withconventionalTRA(Table I). A1:1 randomized study fromGreece included 200pa- tients undergoing percutaneous coronary angiography through conventional TRA or DRA.45 A low dose of heparinwasadministeredinallpatientsandhemostasis was performed bymanual compression. Access-related complicationsincludingultrasound-assessedRAOwhich was quite high (5% in DRA group and 9% in conven- tional TRA group) but did not differ between the 2 groups.
TheDorsalRadialArteryAccessVersusClassicalRadial Artery Access for Percutaneous CoronaryAngiography (DORA)trialrandomized970patientsundergoingcoro- naryangiographyat3Indiancenters.46 Therateoffore- armRAOat12hwas2%intheDRAgroupand13%inthe conventional TRA(P< .0001).Theincidence ofradial arteryspasmwassignificantlylowerintheDRAgroup, whereastherateofhematomadidnotdifferbetweenthe
2groups.Notably,inthisstudyhemostasiswasachieved withan elastic hemostatic bandage inthe DRA group, andanair-filledcompressiondeviceintheconventional TRAgroup.
In a small study from China, 80 patientsundergoing coronary angiographywere assignedto DRA orTRA.47 Hemostasiswas achievedinall patientswithan elastic hemostaticbandageandRAOwasreportedinonly1pa- tientintheconventionalTRAgroup(2.5%vs0%inDRA group,P=.31).
Inasingle-centerrandomizedtrialfromChina,620pa- tient undergoing PCI were dividedin 2 group accord- ingtoaccesssite:312underwentconventionalTRAand 308 underwent DRA.48 The rate of RAO prior to dis- charge assessed by vascular ultrasound occurred in 6 (1.9%)patients inthe DRA group and in 16 (5.2%) in theconventionalTRAgroup(P=.031).Nodifferences wereobserved intherate of otheraccess-relatedcom- plications. Similarly, hemostasis was achieved with an elastic hemostatic bandage in the DRA group, and an air-filled compression device in the conventional TRA group.
TableI. Publishedrandomizedstudiescomparingdistalradialaccesswithconventionaltransradialaccess
Study Y Sites Country Patients
(n)
Primary outcome
Hemostasis RAO
assessment RAO inDRA group
RAOin TRAgroup
P-value
Koutouzis etal.45
2019 1 Greece 200 Access
switch
Manualcompression Vascular ultrasound
5% 9% .407
Sharma etal.46 (DORA)
2020 3 India 970 Multiple
endpoints
Air-filledCompression deviceafterTRA, elastichemostatic bandageafterDRA
Pulse Palpation
2% 13% <.0001
Luetal.47 2020 1 China 80 Undetailed Elastichemostatic bandage
Vascular ultrasound
0% 2.5% .31
Wang etal.48
2020 1 China 620 Multiple
endpoints
Air-filledcompression deviceafterTRA, elastichemostatic bandageafterDRA
Vascular ultrasound
1.9% 5.2% .031
Linetal.49 2020 1 China 900 Access
success
Dedicatedhemostatic deviceafterTRA, elastichemostatic bandageafterDRA
Vascular ultrasound
1.56% 3.78% .035
Eid-Lidt etal.50 (DAPRAO)
2021 1 Mexico 282 RAOat24
h
Air-filledCompression device
Vascular Ultrasound
0.7% 8.4% .002
Inanothersingle-centerrandomizedtrialfromChina, 900patients undergoing a percutaneous coronary pro- cedurewererandomizedtoconventionalTRAorDRA.49 The rate of RAO prior to discharge assessed byvascu- larultrasoundoccurredin7(1.6%)patientsintheDRA groupandin17(3.8%)intheconventionalTRAgroup (P=.033).Therateofhematomadidnotsignificantlydif- ferbetweenthe2groupswhiletheincidenceofaccess sitebleedingwassignificantlylowerintheDRAgroup.
Hemostasiswasachievedwithanelastichemostaticban- dageintheDRA groupanda dedicatedhemostaticde- viceintheconventionalTRAgroup.
TherecentlypublishedDistalRadialApproachtoPre- ventRadialArteryOcclusion(DAPRAO)wasaprospec- tive,randomized,single-centerMexicanstudy,inwhich patientsundergoingapercutaneouscoronaryprocedure were randomly assigned (1:1) to conventional TRA or DRA.50 Theprimaryoutcomeofforearm RAO assessed byvascularultrasoundat24hoccurredin1(0.7%)of140 patientsintheDRAgroupcomparedto12(8.4%)of142 patientsintheconventionalTRAgroup(oddsratio12.8, P=.002)intheperprotocolanalysis.The24hforearm RAOrateintheintention-to-treatanalysis,andthefore- armRAOratesat30daysforboththeperprotocol,and intention-to-treatanalysesshowedsimilarimprovedout- comes withDRA. Importantly, thecrossoverrate from DRAtoTRAwashigh(13.3%),whilethecrossoverrate fromTRAtoDRA wasonly0.7%(P<.001). Nosignif- icantdifferences were found between the 2groups in theincidenceofforearmandhandhematomaandradial arteryspasm.
OverallresultsofcomparativeassessmentsofDRAand TRAare farfrombeingconclusive. Relevantshortcom-
ingsaffectingthesestudiesincludeasingle-centerdesign inallbutoneofthem;anheterogenoushemostasistech- nique(evenwithinthesametrial)thatisnotorientedto RAOprevention;anessentiallyhighrateofRAOandits inconsistentdefinitionacrossthestudies.TheDAPRAO trialistheonlyrandomizedstudyofDRAversusconven- tionalTRAincluding forearm RAO astheprimary end- point.Yet,it is similarly limitedbyits single-centerde- signand byahighrate offorearm RAO intheconven- tionalTRA groupdespite theuse ofpatent hemostasis andslendersheaths,whichisincontrastwithrecenttri- alsusing bestpreventionmethods showinglowerRAO rates,hencequestioningtheexternalvalidityofitsfind- ingsinamorecontemporaryinterventionalpractice.51 , 52
Studymethods Studyobjectiveanddesign
The DIStal vs COnventional RADIAL access (DISCO RADIAL)trialis aprospective, multicenter,openlabel, randomized, controlled study designed to demonstrate thesuperiorityof DRA comparedto conventional TRA with respect to the incidence of forearm RAO at dis- charge.Up to 1300eligible patientswho willundergo adiagnosticcoronaryangiographyand/oraPCIusinga 6FrGlideSheathSlender(TerumoEurope,Leuven, Bel- gium)asthestandardaccesssheathwillberandomlyal- locatedina 1:1ratio toDRAversus TRA.Centersfrom EuropeandJapanwillparticipateonlyifproficientwith DRA.ThestudyoutlineisshowninFigure2.Follow-up is setuntil discharge. The study willbe conducted ac- cordingtotheDeclarationofHelsinkiandapprovalfrom eachcenter’sethicalcommitteewillhavetobeobtained
Figure2
OutlineoftheDISCORADIALtrial.Real-worldpatients(n=1300)willbeenrolledfollowingcompliancetolimitedselectioncriteria(see TableII),indicationtocoronaryangiographyorpercutaneouscoronaryinterventionandsuitabilitytobothdistalradialaccess(DRA)and conventionaltransradialaccess(TRA).Afterwards,patientswillberandomized1:1tooneoranotheraccess,andwillbefollowed-upuntil hospitaldischarge.Ultrasound-assessedradialarteryocclusionat8to48histheprimaryendpointofthestudy.
beforestartingpatientenrolment.TheClinicalTrials.gov identifierisNCT04171570.
Studypopulationandfollow-up
Inclusionand exclusion criteria have beenrestricted (Table II)toenroll a broadpatientpopulation withan indication for coronary angiography and/or a PCI rep- resentativeofroutineclinicalpractice.Patientsaged18 yearsorolder,whohaveprovidedwritteninformedcon- sent andwhoare suitablefor bothDRA andTRAwith the6FrGlideSheathSlenderareeligibleforenrolment.
Exclusioncriteriaaremedicalconditionsthatmaycause non–compliance with the study protocol and/or may confound the data interpretation, patients on chronic hemodialysis,presentingwithST-elevatedmyocardialin-
farctionorundergoing PCI forchronic total occlusion.
Patients will be followed-up for the prespecified end- pointsuntilhospitaldischarge,and thereare nosched- uledfollow-upcontactsafterhospitaldischarge.
Radialsheath
The 6FrGlideSheathSlender isa 6Fr-compatiblera- dialsheathwithahydrophiliccoatingandhasespecially beendesignedtoprovideaccesstosmallerarteries.The outerdiameterhasbeenreducedfrom2.63mmto2.46 mmthroughareductioninwallthicknessfrom0.20mm to0.12mm.53 Thiswallthicknessisthinnerthancurrent non–Slender6Frsheaths.Theinnerdiameterhasbeen
TableII. DISCORADIALinclusionandexclusioncriteria Inclusioncriteria
Aged≥18y
Signedinformedconsentform
IndicationtodiagnosticcoronaryangiographyorPCI
Patient’swillingnesstocomplywithallprotocol-requiredevaluationsduringthehospitalization Patient’ssuitabilityforbothDRAandconventionalTRAusing6FrGlideSheathSlender Exclusioncriteria
Medicalconditionthatmaycausenon–compliancewiththeprotocoland/orconfoundthedatainterpretation Chronichemodialysis
ST-elevatedmyocardialinfarction(STEMI)
Treatmentofacoronarychronictotalocclusion(CTO)lesion
maintainedat2.22mmtoallowcompatibilitywithall6 Frdevices.
Randomizationandarterialaccessprocedure Concealedallocationof studytreatment isto beper- formed via a Web-based interactive randomization sys- temavailableathttps://secure.eclinicalos.com.Random- ization is achieved with computer-generated random sequence with a random block size stratified at site level.
For both patients randomized to DRA or TRA, intra- venousaccess,preferablyinthecontralateralarmforthe administration of medications is recommendedfor the administrationofmedications.Thechoiceofrightorleft radialarteryis leftto thediscretion oftheoperator,as wellas the use of ultrasound to guide theaccess pro- cedure.Afterlocalanesthesia,eithertheSeldingerorthe modified-Seldingertechniqueisusedtoobtainarterialac- cess.AfterplacementoftheGlideSheathSlender,acock- tailof5mgverapamil,and100or200mgnitroglycerine isadministeredtopreventarterialspasm.Administration anddosageofheparinandotheranti–thromboticagents isperhospitalroutine.Iftheinitialattempttoobtainvas- cularaccessattherandomizedaccesssite(DRAorTRA) fails,allfurtherattemptswillbeconsideredascross-over, andincludetheuseofthecontralateralarmorotherar- teries(femoralorulnarartery)orcross-overtotheother group.ForTRA,thepatient’shandispositionedinanex- tendedposition withthepalm positionedsupinated.It is advisedto puncture theradial artery2cmproximal to the styloid process of the radial bone witha 30 to 45°entryangletotheskin.ForDRA,thepatient’shand ispositionedwiththeanatomicsnuffboxupward.After confirmingbymanualpalpation,thepresenceofawell- developeddistalradialarteryintheanatomicalsnuffbox orthedorsumofthehand,thearteryispuncturedwith 30to45°entryangletotheskininthedirectionofthe strongest pulse. The anterior wall puncture technique ispreferred, butthethrough-and-throughpuncture can alsobeused.24 Inbothcases,carefulmanipulationofthe needle is advised to avoid touching theperiosteum of thescaphoidortrapeziumbones,asthiscanbepainful.
Aftersuccessfularterialpuncture,therestoftheaccess procedureissimilarasforTRA.
Hemostasisprotocol
For patients in whom arterial access is obtained throughtheconventionalTRAmethod,hemostasiswith aclosuredevice isrecommendedwithpatenthemosta- sisimplementedaccordingtothePROPHETstudyproto- col.18 Briefly,afterplacementofthehemostaticcompres- siondeviceandremovalofthesheath,hemostaticpres- sureissettoaleveljustenoughtomaintainhemostasis withoutcompromisingradialarterypatencyasassessed by thereverse Barbeau test. This is performed by ob- servationofthepulsatilewaveformsfromaplethysmo- graphicsensorplacedontheindexfingeraftercompres- sionoftheulnarartery.Absenceofaplethysmographic waveformindicatesocclusivecompressionoftheradial arteryandthepressureinthehemostaticdeviceshould graduallybereduced untilreturnof thewaveform. For patients who received DRA, access site closure, and hemostasis are per hospital practice. Details regarding hemostasistechniques and protocols will be collected foreverypatient.
Operatorcriteriaforeligibility
ConventionalTRAandDRArequirebothspecificskills anddedicatedtraining.Thepresentstudyisnotaimedat investigatingthelearningcurveofDRA,ratherassessing thecomparativeefficacy,andsafetyofDRAversusTRA byfullytrainedinterventionalcardiologistswitheffective operatingexperiencewithbothaccesses.Hence,single operatorsqualifyforthestudyproviding:(1)theyareex- periencedoperatorsregularlyperformingtransradialPCI inthewholespectrumofcoronaryarterydisease,includ- ingACS, (2)they are fully independentwith DRA, (3) theyhaveperformeda minimumof100procedures by DRA.
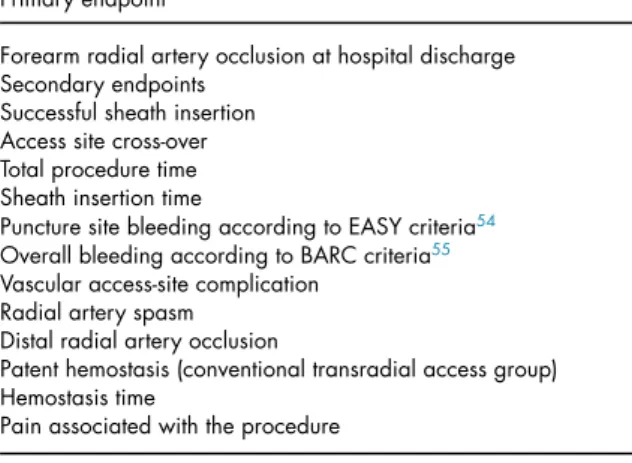
Studyendpoints
TheprimaryendpointoftheDISCORADIALtrialisthe incidenceofforearmRAOathospitalizationdischargeas-
TableIII. DISCORADIALEndpoints Primaryendpoint
Forearmradialarteryocclusionathospitaldischarge Secondaryendpoints
Successfulsheathinsertion Accesssitecross-over Totalproceduretime Sheathinsertiontime
PuncturesitebleedingaccordingtoEASYcriteria54 OverallbleedingaccordingtoBARCcriteria55 Vascularaccess-sitecomplication
Radialarteryspasm Distalradialarteryocclusion
Patenthemostasis(conventionaltransradialaccessgroup) Hemostasistime
Painassociatedwiththeprocedure
BARC, Bleeding Academic Research Consortium; EASY, Early Discharge after Tran- sradial Stenting of Coronary Arteries Study
sessedbyanindependentinvestigator,whowasnotin- volvedintheprocedure. Thepresenceorabsenceofa duplexultrasound anterogradeflow signal distalto the radialarteryaccesssiteischeckedaccordingtohospital routine,ideallybetween 8to48hourspost-procedure.
Thearteryisconsideredoccludedifnoflowsignalcanbe detected.ForpatientsassignedtoDRA,boththeforearm and the distalartery are assessed. The secondary end- points are listed inTable III. Endpoint’sdefinitions are fullydetailedinAppendix.
Statisticalmethods
The primary hypothesis of the study is that DRA is superiorto conventional TRAwith respect tothe inci- denceofforearmRAOatdischarge.FortheTRAgroup, theassumptionis that3.5%of thepatientswillexperi- enceaRAObasedupondataoftheGlidesheathSlender 6FrsubgroupfromtheRAPandBEAT study.20 Forthe DRAgroup,anincidenceofforearmRAO of1.0%isas- sumed,basedonnumerouspreviousstudies. Fora sta- tisticalpowerof 80%anda 2-sidedalphaerrorof0.05, assumingacross-overrateof10%andadrop-outrateof 5%, 648patientsper group areneeded. The totalsam- plesizewasthereforesetto1300patients.Theprimary endpoint analysis will be performed on the intention- to-treat(ITT)population,ie,baseduponrandomization assignmenttoeither theTRAortheDRA group.Atip- ping pointanalysis willbeperformed shouldthenum- berofmissingdataexceed15%to20%,althoughnotex- pectedbecauseoftheshortobservationperiod.Forthe secondaryendpointanalyses,thesafetyanalyseswillbe performedontheas-treated populationonly,while the efficacyanalyseswillbeperformedontheITT,andthe per-protocol (PP)populations. The PPpopulation will exclude patients who crossedoveror hadmajor viola- tionstothestudyprotocol.Normalityofdatawillbeas- sessed with the Shapiro-Wilktest and continuous vari-
ableswillbereportedasmeanandstandarddeviationor asmedian (interquartilerange) if skewed. Comparison ofcontinuousvariableswillbeperformedwiththeStu- dentttestorMann-Whitneytest,asappropriate.Catego- rialvariableswillbereportedascount(percentages)and comparativetestingwillbeperformedwiththeχ2 tests orFisher exacttest,asappropriate.Assensitivityanaly- ses,logisticregressionwillbecarriedouttoestimateodd ratios,and95%confidenceintervalcomparingthetested treatmentoptions.Toevaluateforconsistencyofresults amongsubgroupsofinterest,exploratorysubgroupanal- ysesarepre-specified(OnlineAppendix).
Studytimelines,datamonitoringandfundingsource The first patient was randomizedat thecoordinating centerinDecember2019,andthestudy wasprojected tobecompletedwithin1year.Becauseofthenegative impactofCOVID-19pandemicsoncatheterizationlabo- ratoriesactivity andtheoverallreassignmentof health- careworkers,studyenrolmentwassignificantlyslowed witha correctedestimate of endingenrollment at the endoftheSummerof2021.
The DISCORADIALtrialissponsoredbyTerumoEu- rope which is responsible for the study management, risk-baseddata monitoring, and statisticalanalysis.The supportivecompanyhasnoroleindesignof thestudy and publication of the paper reporting thefinal study findings.
Discussion
Theannualmedianofover5,000diagnosticcoronary angiographiesandover2,400PCIsbothpermillionpeo- plereportedforsixteenESCmember countriespartici- patingintheEuropeanAssociationofPercutaneousCar- diovascularInterventions (EAPCI)Atlas surveyof 2016 indicatethelargescaleonwhichthese proceduresare performed annually and reinforce the importance of achievingsafearterialaccesstothecoronaryarterysys- tem.56 Inthatperspective,greatprogresshasbeenmade overthe last 3 decades with thedevelopment of TRA whichhasbecomethedefaultaccess methodforcoro- nary procedures, unless there are overriding procedu- ralconsiderations.1-4 WiththeadventofTRA,dedicated equipmenthasbeen developedto furtherimprove the accesssuccessrate,hemostasisandproceduralsafety,in- cludingguidecatheters,hemostasisdevicesandvascular sheathswithasmaller outerdiameterto accommodate thesmaller diameter ofthe radialartery.20 , 53 All inall, thesedeviceshavepromotedaprogressivereductionin RAO that howeverstill remains themajorlimitation of TRA.15
Against this background, DRA has enthusiastically emerged as an alternative access pledging to virtually cancel RAO.22 , 24 The feasibility and safety of DRA has been demonstrated in observational registries27-44 and
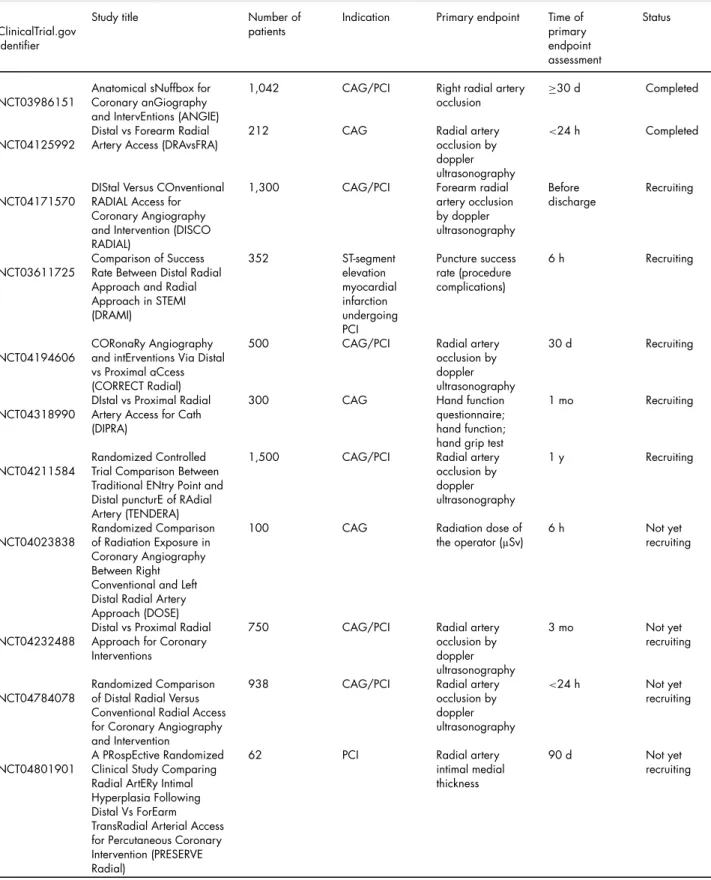
TableIV. Overviewofregisteredrandomizedtrialcomparingconventionaltransradialaccessversusdistalradialaccess
ClinicalTrial.gov identifier
Studytitle Numberof
patients
Indication Primaryendpoint Timeof primary endpoint assessment
Status
NCT03986151
AnatomicalsNuffboxfor CoronaryanGiography andIntervEntions(ANGIE)
1,042 CAG/PCI Rightradialartery
occlusion
≥30d Completed
NCT04125992
DistalvsForearmRadial ArteryAccess(DRAvsFRA)
212 CAG Radialartery
occlusionby doppler ultrasonography
<24h Completed
NCT04171570
DIStalVersusCOnventional RADIALAccessfor CoronaryAngiography andIntervention(DISCO RADIAL)
1,300 CAG/PCI Forearmradial
arteryocclusion bydoppler ultrasonography
Before discharge
Recruiting
NCT03611725
ComparisonofSuccess RateBetweenDistalRadial ApproachandRadial ApproachinSTEMI (DRAMI)
352 ST-segment
elevation myocardial infarction undergoing PCI
Puncturesuccess rate(procedure complications)
6h Recruiting
NCT04194606
CORonaRyAngiography andintErventionsViaDistal vsProximalaCcess (CORRECTRadial)
500 CAG/PCI Radialartery
occlusionby doppler ultrasonography
30d Recruiting
NCT04318990
DIstalvsProximalRadial ArteryAccessforCath (DIPRA)
300 CAG Handfunction
questionnaire;
handfunction;
handgriptest
1mo Recruiting
NCT04211584
RandomizedControlled TrialComparisonBetween TraditionalENtryPointand DistalpuncturEofRAdial Artery(TENDERA)
1,500 CAG/PCI Radialartery
occlusionby doppler ultrasonography
1y Recruiting
NCT04023838
RandomizedComparison ofRadiationExposurein CoronaryAngiography BetweenRight ConventionalandLeft DistalRadialArtery Approach(DOSE)
100 CAG Radiationdoseof
theoperator(µSv)
6h Notyet
recruiting
NCT04232488
DistalvsProximalRadial ApproachforCoronary Interventions
750 CAG/PCI Radialartery
occlusionby doppler ultrasonography
3mo Notyet
recruiting
NCT04784078
RandomizedComparison ofDistalRadialVersus ConventionalRadialAccess forCoronaryAngiography andIntervention
938 CAG/PCI Radialartery
occlusionby doppler ultrasonography
<24h Notyet
recruiting
NCT04801901
APRospEctiveRandomized ClinicalStudyComparing RadialArtERyIntimal HyperplasiaFollowing DistalVsForEarm TransRadialArterialAccess forPercutaneousCoronary Intervention(PRESERVE Radial)
62 PCI Radialartery
intimalmedial thickness
90d Notyet
recruiting
CAG, coronary angiography; PCI, percutaneous coronary intervention
Figure3
RadialarteryocclusionpreventivemeasuresintheDISCORADIALtrial.
a decentnumber ofrandomized studies45-49 comparing DRA versus TRAareeither ongoing orhave beenpub- lishedtoindicatethescientificinteresttoinvestigatethis emergingarterialaccessmodality.Anoverviewoftheon- goingrandomizedtrialcomparingTRAversusDRAreg- isteredonClinicalTrial.gov isprovidedinTableIV.The primaryendpointofthemajorityofthesestudiesisRAO assessedbyduplexultrasound.Thetimepointofassess- mentvariesfrom<24hoursto1-yearpost-procedureand thesamplesizesvarybetween212and1,500patients.
DISCORADIALemergesasthefirstlarge-scaleinterna- tionalrandomizedcontrolledtrialdesignedtoinvestigate thebenefits ofDRA over conventional TRA, appearing unique inseveral respects.First, theparticipating cen- ters are highly proficient with transradial practice and allqualifyingoperatorshavetoprovideextendedexpe- riencewithbothconventionalTRAandDRA.Moreover, sincetheradialarterybecomestheaccesssiteofchoice foranincreasingnumberofindicationsandtheneedfor RAO prevention is bound to grow in the near future, the study protocolmandates therigorous implementa-
tioninthecatheterizationlaboratoryofbestpracticeto reduceRAOassummarizedinFigure3.Notably,theuse of thethin-walled 6 Fr GlideSheath Slender,that is es- peciallyvaluedintheslightlysmallerdistalradialartery, has been set as the default sheath for both TRA, and DRAinordertoexcludesthevariationinaccessdevices asconfoundingfactor.Indeed,to fullyunraveltherole ofDRA,DISCORADIALhasbeendesignedto compare thisnewer access withTRAimplementing optimal, up todate,evidence-basedcaretopreserveradialarterypa- tency.Hence,theRAOrateintheconventionalgrouphas beenestimatedintermsof3.5%,afigurethatissubstan- tiallylowerthanthegoalsuggestedbytherecentInterna- tionalConsensusStatementonthepreventionofRAOfor internalqualitycontrolofeverytransradial programs.15 Yet,thedefinitionofRAOisveryconservative,requiring systematicvascularultrasoundassessmentinallpatients within48hours.Thesamplesizeissufficientlylargeto yieldanadequatelypoweredmulticentertrialcomparing DRAwithconventionalTRAaccordingtoarandomized designresultsinareal-worldsetting.
Finally, multiple, rigorously detailed, relevant sec- ondaryendpointswillalsobeassessed,includingaccess- site cross over, hemostasistime and access-site related complications,andwillreflectthecurrentDRApractice andoutcomeinareal-worldsettingofexperiencedcen- tersandoperatorsusingbothradialaccesstechniques.
Conclusion
DISCO RADIAL is a prospective, multicenter, open- label, randomized,controlled superiority trialdesigned to compare DRA versus TRA with respect to theinci- denceofRAOatdischarge.Thestudyaimsatgenerating reliableclinicalevidenceonthepotentialbenefitsofthis novelapproachovertheconventionalTRA,andtosup- porttheuseofDRAasanalternativetotheconventional TRA.TheprincipalresultsareexpectedinFall2021.
Authors’ contribution
AdelAminian:Conceptualization,Methodology,Inves- tigation, Writing – original draft; Gregory A. Sgueglia:
Conceptualization, Methodology, Investigation, Writing – originaldraft;MarcusWiemer:Investigation,Writing– review&editing;GabrieleLuigiGasparini:Investigation, Writing– review & editing; Joelle Kefer: Investigation, Writing– review&editing;ZoltanRuzsa:Investigation, Writing– review&editing;MaartenA.H.vanLeeuwen:
Investigation, Writing – review & editing; Bert Vande- loo: Investigation, Writing– review & editing, Claudiu Ungureanu: Investigation, Writing – review & editing;
SaskoKedev:Investigation,Writing– review&editing, Juan F Iglesias: Investigation, Writing – review & edit- ing;GregorLeibundgut:Investigation,Writing– review
& editing;KarimRatib:Investigation, Writing– review
&editing;IvoBernat:Investigation,Writing– review&
editing;IreneBarriocanal:Conceptualization,Methodol- ogy,Investigation,Writing– review&editing;Vladimir Borovicanin:Conceptualization,Methodology,Investiga- tion,Writing– review&editing;ShigeruSaito:Concep- tualization,Methodology,Investigation,Writing– review
&editing.
Funding
ThisstudyissponsoredandfundedbyTerumoEurope, Leuven,Belgium.
Conflictof interest
IBandVBare full-timeemployeesofTerumo Europe N.V.Theotherauthorsreportnoconflictofinterest.
Acknowledgments
TheauthorsthankTerumoEuropefortheeditorialas- sistanceinthepreparationofthismanuscript.
Supplementarymaterials
Supplementarymaterialassociatedwiththisarticlecan be found, in the online version, at doi:10.1016/j.ahj.
2021.10.180.
References
1. NeumannFJ,Sousa-UvaM,AhlssonA,etal.2018ESC/EACTS Guidelinesonmyocardialrevascularization.EurHeartJ 2019;40:87–165.
2. IbanezB,JamesS,AgewallS,etal.2017ESCGuidelinesfor themanagementofacutemyocardialinfarctioninpatients presentingwithST-segmentelevation:TheTaskForceforthe managementofacutemyocardialinfarctioninpatientspresenting withST-segmentelevationoftheEuropeanSocietyofCardiology (ESC).EurHeartJ2018;39:119.
3. ColletJP,ThieleH,BarbatoE,etal.2020ESCGuidelinesforthe managementofacutecoronarysyndromesinpatientspresenting withoutpersistentST-segmentelevation.EurHeartJ
2021;42:1289.
4. MasonPJ,ShahB,Tamis-HollandJE,etal.Anupdateonradial arteryaccessandbestpracticesfortransradialcoronary angiographyandinterventioninacutecoronarysyndrome:a scientificstatementfromtheamericanheartassociation.Circ CardiovascInterv2018;11.
5. JollySS,YusufS,CairnsJ,etal.Radialversusfemoralaccessfor coronaryangiographyandinterventioninpatientswithacute coronarysyndromes(RIVAL):arandomised,parallelgroup, multicentretrial.Lancet2011;377:1409.
6. ValgimigliM,GagnorA,CalabroP,etal.Radialversusfemoral accessinpatientswithacutecoronarysyndromesundergoing invasivemanagement:arandomisedmulticentretrial.Lancet 2015;385:2465.
7. FerranteG,RaoSV,JuniP,etal.Radialversusfemoralaccessfor coronaryinterventionsacrosstheentirespectrumofpatientswith coronaryarterydisease:ameta-analysisofrandomizedtrials.
JACCCardiovascInterv2016;9:1419.
8. MeijersTA,AminianA,vanWelyM,etal.Randomized comparisonbetweenradialandfemorallarge-boreaccessfor complexpercutaneouscoronaryintervention.JACCCardiovasc Interv2021;14:1293–303.
9. CooperCJ,El-ShiekhRA,CohenDJ,etal.Effectoftransradial accessonqualityoflifeandcostofcardiaccatheterization:a randomizedcomparison.AmHeartJ1999;138:430. 10.AminAP,PattersonM,HouseJA,etal.Costsassociatedwith
accesssiteandsame-daydischargeamongmedicare
beneficiariesundergoingpercutaneouscoronaryintervention:an evaluationofthecurrentpercutaneouscoronaryinterventioncare pathwaysintheUnitedStates.JACCCardiovascInterv 2017;10:342.
11.RomagnoliE,Biondi-ZoccaiG,SciahbasiA,etal.Radialversus femoralrandomizedinvestigationinST-segmentelevationacute coronarysyndrome:theRIFLE-STEACS(radialversusfemoral randomizedinvestigationinST-elevationacutecoronary syndrome)study.JAmCollCardiol2012;60:2481. 12.TitanoJJ,PatelRS,FischmanAM.Transradialaccessin
interventionalradiology.AdvRadiatOncol2020;2:127. 13.UhlemannM,Mobius-WinklerS,MendeM,etal.TheLeipzig
prospectivevascularultrasoundregistryinradialartery catheterization:impactofsheathsizeonvascularcomplications.
JACCCardiovascInterv2012;5:36–43.