BIOLOGICAL PROPERTIES OF INORGANIC FLUORIDES
T
o THE GENERAL PUBLIC, fluorides are best known for their dangerous properties ; ask the average man what he knows about fluorides and he will probably mention at least two uses : (a) to etch glass, and (b) as a roach powder or as a rat or ant poison. Few people have had any reason to use fluorides for etching glass, but the use of fluorides as insecticides and rodenticides is so widespread that sodium fluoride is almost a common household preparation. The custom of keeping insecticides in the cupboard along with soaps and washing powders, coupled with the innocuous appearance of sodium fluoride—a white powder easily mistaken for powdered milk, baking powder, powdered sugar, corn starch, or pancake flour—is responsible for the many reports in the medical literature of tragic accidents.
This notoriety has colored the biological appraisal of fluorides ; for example, Sollmann (1957) says, ''Sodium fluoride, NaF, is a general protoplasmic poison, of some toxicological importance and considerable scientific inter est.' ' In many cities, the average man today would add a third use of fluorides : water fluoridation to reduce dental caries. A discussion of this use is presented in the chapter "The Effects of Fluorides on Bones and Teeth."
In this chapter, the biological properties of inorganic fluorides will be summarized. The discussion falls easily into two parts: (1) acute poisoning and (2) chronic poisoning. In each part, the literature on human poisonings is presented first, followed by data from studies of experimental animals.
In each part what is known concerning the mechanism of poisoning is given. A discussion of fluoride metabolism concludes this chapter.
The biological effects of the organic fluorides are in most cases not due to the fluoride ion and are so different from those of the inorganic fluorides that a separate volume is devoted to these new and interesting compounds.
One aspect of the biological effects of fluorides has become of sufficient importance to merit a separate and extended presentation: the effects on teeth and bones, the subject of a second chapter. The classic work of Roholm (1937 a) covers the available information up to about 1935 so well that in general only reports since that date are mentioned in the bibliographies for each of the two chapters. Against Roholm's scholarly summary as a back
drop, the more recent evidence has been organized and tabulated in an identical framework, partly in tribute to Roholm's excellence of presenta
tion and partly for ease of use. Thus, to obtain an inclusive picture of acute
1
human poisonings by fluorides, it is possible to combine Roholm's section under that title with the appropriate sections of this chapter; the table forms have been preserved in many instances to facilitate such combina
tions.
Our purpose has been to collect the information about the biological effects of fluorides into a compact form. We have adopted the practice of tabulating information rather than making prose abstracts. Certain points have been expanded upon in the text, sometimes because the point is inherently important, sometimes because we were interested in the matter. We have not attempted to formulate and state a critical opinion of the knowledge about every biological effect of fluorides. The reader with a specific question to answer will find help, we hope, in the tables and the bibliography, both of which are intended to be inclusive. Not every pub
lished datum has been tabulated, however; condensations where practicable and at least sample data are presented sufficient to indicate the nature of the study. The number of papers appearing currently on various aspects of this field is large enough to make up-to-date summaries difficult to prepare. A larger number of scientific reports on the biological effects of fluorides has appeared in the past 27 years than in the preceding 75 years reviewed by Roholm.
Acute Effects of Inorganic Fluorides
FATAL H U M A N POISONINGS
A brief résumé of the salient features of acute human poisoning will serve as an introduction to the lengthy list of poisonings. After a large dose of a soluble fluoride is ingested, accidentally or by suicidal intent, there follows a catastrophic symptom train. The course of poisoning is violent and brief; deaths are frequently recorded in 2-4 hours. A "large" dose means a teaspoonful or more (5-10 gm) of sodium fluoride. The exact cause of death is still obscure.
Description of an Extraordinary Mass Poisoning
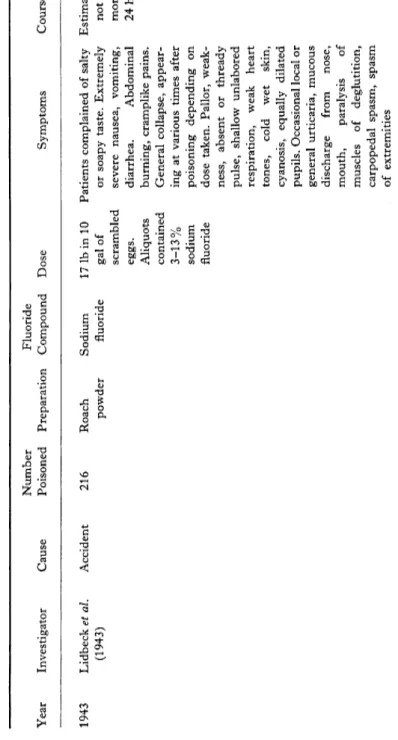
The accidental ingestion of sodium fluoride at the Oregon State Hospital, described by Lidbeck et al. (1943) produced the highest morbid
ity and mortality ever reported in a single episode. Following an evening meal of scrambled eggs, there were 263 cases of acute poisoning; 47 termi
nated fatally. "When toxicologic examination revealed the presence of sodium fluoride, it was apparent that roach powder had been placed in the scrambled eggs served at the evening meal. Subsequent investigation disclosed that a patient helper had unwittingly mistaken roach powder for
powdered milk and had added approximately 17 pounds of the compound to a 10-gallon mixture of scrambled eggs. Fortunately the eggs were not generally distributed throughout the hospital but were served to only five of the working wards.
"The food was rejected by many of the patients because of a salty or soapy taste, while others complained of numbness of the mouth. Extremely severe nausea, vomiting and diarrhea occurred abruptly and at times simultaneously, and blood was noted in the vomitus and stools in many instances. Soon after the meal there were complaints of abdominal burning and cramplike pains. General collapse developed in most instances but at variable periods of time, apparently depending on the concentration of the poison. This was characterized by pallor, weakness, absent or thready pulse, shallow unlabored respiration, weak heart tones, wet cold skin, cyanosis and equally dilated pupils. When this picture was pronounced, death almost invariably occurred. Local or generalized urticaria occurred in some instances, while in others there was a thick mucoid discharge from the mouth and nose. When death was delayed, and in some cases in which recovery occurred, there were paralysis of the muscles of deglutition, carpopedal spasm and spasm of the extremities. Convulsions and abdominal tenderness and rigidity were absent. In the majority of cases, death occurred between two and four hours after ingestion of the food, although in a few instances death was delayed for eighteen or twenty hours."
Compilation of Fatalities
Roholm (1937 a) summarized the available data by listing 60 fatal cases of poisoning that were reported during the interval 1873-1935. The symp
toms most frequently seen were vomiting, abdominal pains, diarrhea, and convulsions and spasms, in that order. In 30 of 32 cases brought to autopsy examination, inflammatory or corrosive changes in the stomach were described; similar but less severe changes were evident in the small intestine.
The trend, noted by Roholm (1937 a), toward an increasing frequency of acute poisoning is still apparent. In the interval 1873-1917, the number of deaths was 6, and in the period 1918-1935, the total rose to 54. Roholm suggests that the true number of such poisonings was greater, inasmuch as some cases may not have been correctly identified. During 1939-1957 (Table I) a total of 93 fatal cases was reported in more or less detail in the readily available medical literature. During the 6 years from 1950 through 1955, an additional 34 accidental deaths were reported in the U.S. (Table II). In 11 recent years (1944-1955) there were 68 such deaths as con
trasted with the 60 deaths recorded by Roholm in 62 years.
TABLE I ACUTE FATAL FLUORIDE INTOXICATIONS, 1935-1957 Year Investigator Cause Sex and age Preparation used Fluoride compound Dose Duration 1936 J. L. Carr (1936) Suicide — Insecticide? Sodium fluoride Less than Overnight 28 gm CLINICAL SYMPTOMS : — NECROSCOPY RESULTS : Fluoride found in stomach 1936 J. L. Carr (1936) Suicide — Insecticide? Sodium fluoride Less than Overnight 28 gm CLINICAL SYMPTOMS : — NECROSCOPY RESULTS: Fluoride found in stomach 1936 Geiger (1936) Accident M 87 yr Mislabeled Sodium fluoride ca. 3-4 gm Less than J. L. Carr (1936) baking soda 12 hr CLINICAL SYMPTOMS: Vomiting; severe pain over chest; perspiration; diarrhea; exudate from nose; loss of power in extremities; collapse NECROSCOPY RESULTS: Extraordinary congestion; hemorrhagic infiltration all organs especially lung, spleen. Lung: no necrosis. Heart: cardiovascular beds congested, loss muscle tone, moderate dilation. Liver: yellow, no necrosis but cloudy swelling. Spleen: enlarged, engorged with erythrocytes. Pancreas: grossly normal. Kidneys: congested, edematous, moderately swollen. Gastrointestinal tract: acutely congested ; gastric mucosa hyperemic with small points of hemorrhage. Similar less severe changes in rest of bowel 1936 Geiger (1936) Accident F 61 yr Mislabeled Sodium fluoride ca. 3-4 gm 6J hr J. L. Carr (1936) baking soda CLINICAL SYMPTOMS: NO vomiting; rapid prostration, feverish; nausea; diarrhea; severe oral burnings, sore tongue; very weak; pre monition of death; fluoride found in stomach; also 250 ppm arsenic from bottle NECROSCOPY RESULTS : As in above case
1936 Geiger (1936) Accident F 53 yr Mislabeled Sodium fluoride ca. 3-4 gm 8 hr J. L. Carr (1936) baking soda CLINICAL SYMPTOMS: Perspiration; nausea, vomiting; diarrhea; prostrated; no pulse; abdominal pain; semicomatose; chills; weaker; premonition of death; cramps in legs; clonic spasms; burning sensation "inside"; rash over whole body (attributed to anti-coagulant effect of fluoride) ; death from respiratory failure NECROSCOPY RESULTS: Extraordinary congestion; hemorrhagic infiltration all organs, especially lung, spleen. Lung: no necrosis. Heart: cardiovascular beds congested, loss muscle tone, moderate dilation. Liver: yellow, no necrosis but cloudy swelling. Spleen: enlarged, engorged with erythrocytes. Pancreas: grossly normal. Kidneys: congested, edematous, moderately swollen. Gastrointestinal tract: acutely congested; gastric mucosa hyperemic with small points of hemorrhage. Similar, less severe changes in rest of bowel 1937 Robbers (1937) CLINICAL SYMPTOMS: — NECROSCOPY RESULTS : —
Suicide M 'Servus- Sodium Estd. 40 gm > 30 min schwabentod ' ' silicofl uoride
Ο a Η M
η
w ο m Ο g •ζ Ο f d Ο 2 51937 Schôneberger (1937) Accident CLINICAL SYMPTOMS : — NECROSCOPY RESULTS: 3 deaths
M Disinfectant "Montanin" 30% fluorosilic acid 1937 Schôneberger (1937) Accident CLINICAL SYMPTOMS : — NECROSCOPY RESULTS : —
Child Rodenticide 53% sodium silicofluoride 1937 Wirthlin (1937) Suicide F 17 yr — Sodium fluoride ca. 225 gm 2J hr CLINICAL SYMPTOMS: Nausea; vomiting; diarrhea; epigastric pain; dyspnea; face pale, covered with cold perspiration; conjunctiva mem branes nose and throat swollen, congested; lips swollen; respiration deep, labored pulse rapid; abdomen tender; extremities limp, cyanotic NECROSCOPY RESULTS : Fluoride detected in vomitus. No rigor mortis until 4 hr after death Continued on following page ^
TABLE I (continued) ACUTE, FATAL FLUORIDE INTOXICATIONS, 1935-1957 Year Investigator Cause Sex and age Preparation used Fluoride compound Dose Duration 1938 Heydrich (1938) Accident M 32 yr Rat poison and Sodium Cake icing ca. 24 hr insecticide fluorosilicate prepared containing 4-5% sodium fluosilicate CLINICAL SYMTOMS: Vomiting, diarrhea within hr; colic, muscular weakness in extremities; cramps; cyanosis, circulatory collapse; stupor NECROSCOPY RESULTS: Cerebellum, pons, medulla oblongata gray matter spongy. Negative histology. Heart: bloody coloring (pin head to lens size) on upper left ventricle. Histology negative. Duodenum: digestive brei yellow in color. Stomach: strong folding. Pyloric region: some bleeding. Peripheral vessels, little coagulation. Liver: stasis, hyperemic. Spleen: stasis, hyperemic. Kidney: hyperemic 1938 Heydrich (1938) Accident F 23 yr Rat poison and Sodium As above ca. 19 hr insecticide fluorosilicate CLINICAL SYMPTOMS: Nausea, vomiting in 15-30 min, diarrhea within^hr. Other symptoms as above NECROSCOPY RESULTS: Heart: contracted; no coagulated blood. Lungs: strong odor upon cutting; also in cranial cavity. Lower inferior vena cava: much thin, dark, red blood. Blood contained 0.06 mg fluoride/100 ml; 0.09 mg fluoride/100 gm liver 1938 Heydrich (1938) Accident — As above As above As above — CLINICAL SYMPTOMS : — NECROSCOPY RESULTS : — 1939 Gettlerand — — — — 104 mg — Ellerbrook, (1939) smallest quantity absorbed CLINICAL SYMPTOMS: 5 cases reported; 2 found dead, 3 died within 24 hr NECROSCOPY RESULTS : Cf. Table IVA for tissue analyses
1939 Newspapers Accident M 37 yr — "Soluble Cherry pie fluoride' ' prepared with flour containing 10% F CLINICAL SYMPTOMS: — NECROSCOPY RESULTS: — 1940 Unchecked Accident reference : Food and Drug Review {Jan. 1941) CLINICAL SYMPTOMS: — NECROSCOPY RESULTS: 12 deaths 1940 New York Post Accident F adult (9/5/40) CLINICAL SYMPTOMS : — NECROSCOPY RESULTS : — 1942 Goralewski (1942) Accident M 34 yr — Inhaled hydrogen — 5 days fluoride in industrial plant CLINICAL SYMPTOMS : Numb, excessive thirst, bloody sputum NECROSCOPY RESULTS: Pulmonary abscess, secondary anemia
Sodium fluoride Mistaken for flour in prepar ing pan cakes "Soluble fluoride" Fried eggplant dipped in flour Continued on following page
TABLE I (continued) ACUTE, FATAL FLUORIDE INTOXICATIONS, 1935-1957 Year Investigator Cause Sex and age Preparation used Fluoride compound Dose Duration 1943 Hayhurst (1943) Accident M Insecticide spray Sodium fluoride containing sodium fluoride CLINICAL SYMPTOMS : Death in 5-6 days NECROSCOPY RESULTS : — 1943 Lidbeck et al. Accident 47 cases Roach powder Sodium fluoride Scrambled 2-4 hr for (1943) eggs majority eaten con- 18-20 hr taining 3- for some 13% sodium cases 15 min fluoride one case CLINICAL SYMPTOMS: Patients complained of salty or soapy taste. Extremely severe nausea, vomiting, diarrhea. Abdominal burning. Cramplike pains. General collapse after varying intervals from poisoning, depending upon dose. Pallor, weakness, absent or thready pulse, shallow, unlabored respiration, weak heart tones, cold wet skin, cyanosis, equally dilated pupils. Occasional local or general urticaria, mucous discharge from nose, mouth, paralysis of muscles of swallowing, carpopedal spasms, spasm of extremities NECROSCOPY RESULTS: Stomach, duodenum, first portion oijejunum: mucosa edematous, hyperemic. Stomach contents mucinous, contained large amounts undigested eggs. Colon: empty except for portions undigested food (diarrhea severe); mucosa unchanged. Abdominal viscera; general increased wetness, acute congestion. Liver, Kidney: swollen. Lungs: ballooned at edges, occasional interlobar petechial hemorrhages. No aspiration of stomach contents. Heart: marked dilation of right chambers which contained fluid blood. Brain: slight edema, hyperemia. When death delayed, only other changes were petechial hemorrhages of gastric and duodenal mucosa. Death in 15 min, stomach contents contained 17.2 gm sodium fluoride. Death in 1 hr, contained 3.7 gm sodium fluoride; death in 4 hr, stomach empty: 0.85 gm sodium fluoride in entire liver, 0.21 gm sodium fluoride both kidneys. Death in 18 hr, stomach contained 0.18 gm sodium fluoride. In all cases fluoride shown qualitatively in 10 gm samples, kidney, liver
1943 Liljestrand (1943) Accident F 3 yr 5 mo Rat poison Sodium ca. 0.5-0.7 3 hr silicofluoride gm CLINICAL SYMPTOMS : — NECROSCOPY RESULTS : — 1944 Davydov (1944) Accident — CLINICAL SYMPTOMS : Vomiting. Fluoride in vomitus, gastric fluids NECROSCOPY RESULTS : — 1944 St. Louis Post Accident M 43 yr Dispatch (2/14/44) CLINICAL SYMPTOMS: — NECROSCOPY RESULTS : — 1945 Rabinowitch (1945) Suicide M 39 yr — Sodium fluoride — 3hr 5 min CLINICAL SYMPTOMS: NO vomiting. Salivation; low blood pressure; spasms of hands (carpal spasms of tetany); respiratory failure 2.6 mg Ca/100 ml serum just before death NECROSCOPY RESULTS: Stomach: small area of swelling of mucosa near duodenum 1946 Hulst (1946) Accident — Roach poison — — — CLINICAL SYMPTOMS: 2 deaths NECROSCOPY RESULTS : — 1947 Steenhauer and Accident — Kedde (1947) CLINICAL SYMPTOMS : — NECROSCOPY RESULTS : Cf. Table I VA for tissue analyses
Biscuits 0.2 gm containing NaF per NaF biscuit Sodium fluoride Mistaken for medicine Insecticide 96.7% sodium fluorosilicate "Klakkatox"
Sodium fluorosilicate Bread 18 hr smeared with insecticide Continued on following page
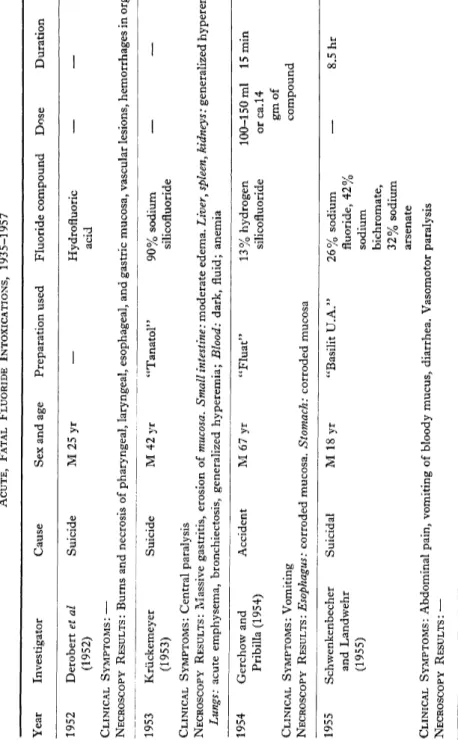
TABLE I (continued) ACUTE, FATAL FLUORIDE INTOXICATIONS, 1935-1957 Year Investigator Cause Sex and age Preparation used Fluoride compound Dose Duration 1952 Derobert et al Suicide M 25 yr — Hydrofluoric — — (1952) acid CLINICAL SYMPTOMS : — NECROSCOPY RESULTS : Burns and necrosis of pharyngeal, laryngeal, esophageal, and gastric mucosa, vascular lesions, hemorrhages in organs 1953 Kruckemeyer Suicide M 42 yr "Tanatol" 90% sodium — — (1953) silicofluoride CLINICAL SYMPTOMS: Central paralysis NECROSCOPY RESULTS: Massive gastritis, erosion of mucosa. Small intestine : moderate edema. Liver, spleen, kidneys: generalized hyperemia; Lungs: acute emphysema, bronchiectosis, generalized hyperemia; Blood: dark, fluid; anemia 1954 Gerchowand Accident M 67 yr "Fluat" 13% hydrogen 100-150 ml 15 min Pribilla (1954) silicofluoride or ca.14 gm of CLINICAL SYMPTOMS : Vomiting compound NECROSCOPY RESULTS: Esophagus: corroded mucosa. Stomach: corroded mucosa 1955 Schwenkenbecher Suicidal M 18 yr "Basilit U.A." 26% sodium — 8.5 hr and Landwehr fluoride, 42% (1955) sodium bichromate, 32% sodium arsenate CLINICAL SYMPTOMS : Abdominal pain, vomiting of bloody mucus, diarrhea. Vasomotor paralysis NECROSCOPY RESULTS : —
T A B L E II
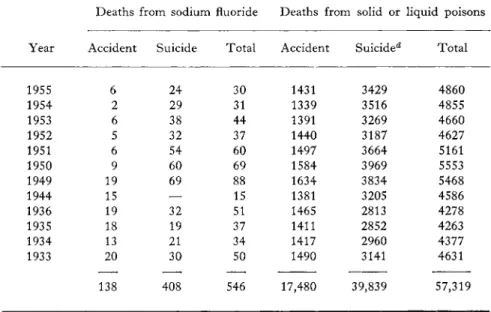
NUMBER OF DEATHS FROM SODIUM FLUORIDE IN THE U . S . IN RELATION TO THE TOTAL NUMBER OF DEATHS FROM PoisoNSa'&>c>
Deaths from sodium fluoride Deaths from solid or liquid poisons
Year Accident Suicide Total Accident Suicide** Total
1955 6 24 30 1431 3429 4860
1954 2 29 31 1339 3516 4855
1953 6 38 44 1391 3269 4660
1952 5 32 37 1440 3187 4627
1951 6 54 60 1497 3664 5161
1950 9 60 69 1584 3969 5553
1949 19 69 88 1634 3834 5468
1944 15 — 15 1381 3205 4586
1936 19 32 51 1465 2813 4278
1935 18 19 37 1411 2852 4263
1934 13 21 34 1417 2960 4377
1933 20 30 50 1490 3141 4631
138 408 546 17,480 39,839 57,319
a Figures not available for missing years.
6 Data for the years 1933-1944 were kindly supplied by Dr. H. L. Dunn, Chief, National Office of Vital Statistics.
c From Mortality Statistics, 1933-36 and Vital Statistics of the United States, 1945 and 1950-55, U. S. Dept. of Commerce, Bureau of the Census.
d All poisons, 1955-1949; solid or liquid posions, 1944-1933.
This striking increase may be ascribed in part to the population in
crease, in part to a better system of recording mortality statistics, and in part to a wider use of fluorides.
In Table III are listed by years the instances of acute, fatal fluoride poisoning occurring in New York City during the interval 1935-1949.
Table II shows similar data for the United States for the years 1933—
1936, for 1944, and for 1949-1955.
To these data can be added the 12 fatal cases reported in Food and Drug Review (Anonymous, 1941) and the 47 cases reported by Lidbeck et al. (1943), none of which is included in these two tables. More than 600 deaths due to inorganic fluoride compounds have occurred in the United States since 1933. Data on a national basis are unavailable for many years during this period. The data for New York City suggest a constant incidence rate for fluoride poisonings. Both in New York City and
T A B L E I I I
ACUTE, FATAL FLUORIDE INTOXICATION, 1 9 3 5 - 1 9 4 9 , N E W YORK CITY»
Cause
Year Suicide Accidental and undetermined Total
1 9 3 5 4 — 4
1 9 3 6 7 3 1 0
1 9 3 7 5 1 6
1 9 3 8 4 3 7
1 9 3 9 3 1 4
1 9 4 0 8 1 9
1 9 4 1 1 0 1 1 1
1 9 4 2 1 1 3 1 4
1 9 4 3 8 4 1 2
1 9 4 4 1 1 1 1 2
1 9 4 5 Not available
1 9 4 6 1 1 — 1 1
1 9 4 7 7 2 9
1 9 4 8 8 2 1 0
1 9 4 9 8 2 1 0
1 2 9
a Unpublished data from Dr. Thomas A. Gonzales, Chief Medical Examiner, City of New York, and Mrs. Billie Weil, of that office (1951).
the country as a whole, the number of deaths due to accidental poisoning is considerably less than that for suicidal deaths. In the entire country, deaths from fluoride poisoning constitute approximately 1% of the total deaths by poisoning. Increased appreciation of the significance of fluorides as toxic agents is attested to by the inclusion for the first time of a category for accidental deaths from fluoride compounds in the Sixth Revision of the International List of Causes of Death, effective in 1949.
Lethal Dose
From a study of the recorded cases a dose range of 5-10 gm of sodium fluoride can be cited as a reasonable estimate of a * 'certainly lethal dose"
for a 70-kg man; this corresponds to 70-140 mg/kg. These data are in excellent agreement with those of Roholm, who reported the smallest single dose of sodium fluoride causing death in the adult man to be about 4 gm. M. M. Black et al. (1949 b) gave a 16-year-old patient suffering
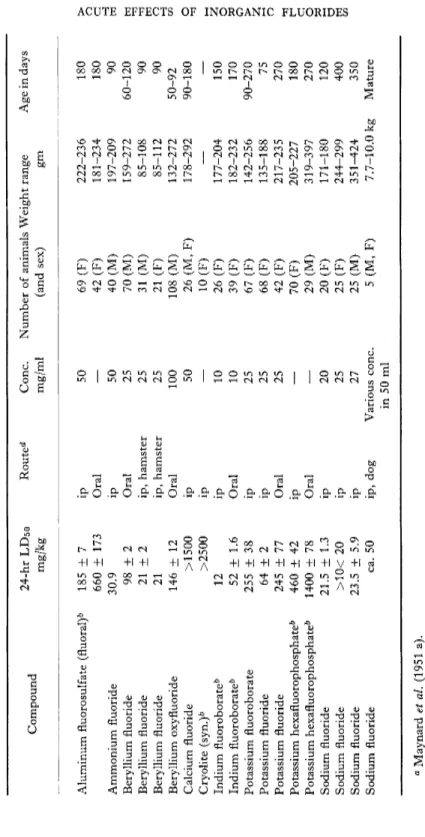
from an adrenal carcinoma an average daily dose of 23 mg/kg of sodium fluoride for nine consecutive days. Although this daily dose is nearly one-third of the minimal estimated single lethal dose, there were no signs of poisoning. This dose is of the same magnitude reported to be lethal for the rat. Data of Maynard et al. (Table IX) establish the 24-hour LD50 dose for sodium fluoride administered intraperitoneally to 171-180 gm female rats as 22 mg/kg; the LDo dose is 15 mg/kg. An increase from 0 to 50%
mortality attended a 25% increase in the dose. The success of Black et al.
in avoiding toxic symptoms (and also the steep slope of the dose-mortality curve in the rat) must stem in considerable part from the rapid removal of fluoride from the body by excretion into the urine and by deposition in the skeleton.
Gettler and Ellerbrook (1939) estimated the smallest absorbed lethal dose of fluoride to be 105 mg in an individual weighing 140 pounds. They reached this estimate by determining chemically the amount of fluoride remaining in the internal organs on a series of five fatal cases. This quantity is exclusive of the fluoride already in the urine or deposited in the skin, nails, hair, fat, or bone. The 105-mg total is much less than that just cited as the ''certainly lethal dose." If 5% of the ingested dose were still present in the viscera at death (a reasonable assumption based on the data of Fig. 1), the original dose would have been more than 2 gm F (or about 4 gm of sodium fluoride). Thus, the figure of 105 mg of fluoride, described as the
"smallest lethal dose of fluoride absorbed" by Gettler and Ellerbrook, is not the lethal dose, nor the total absorbed dose, but represents only the small fraction of the absorbed fluoride still remaining in the soft tissues at death. Therefore, we suggest that the 105 mg F be called the "smallest soft tissue burden" at the time of death from acute fluoride poisoning.
Symptoms
The clinical symptoms of acute poisoning (Table I) are almost without exception those recorded by Roholm. In addition to the symptoms noted by Roholm, single instances are given of a burning sensation in the mouth, a sore tongue, and a lowered blood pressure. In two instances a premonition of death immediately preceded exitus. Nasal discharge was observed in two instances.
The findings at the autopsy examinations were comparable to those given by Roholm.
Time of Death
The course of fatal poisoning is characteristically rapid; death fre
quently occurs in 2-4 hours. In the cases listed by Roholm, death from sodium fluoride occurred at times varying from 45 minutes to 22 hours after
ingestion of the agent. In Table I, the time intervals vary from 15 minutes to about 24 hours. In both series, many deaths occurred in 6-10 hours following ingestion of the poison. If a victim survives the first 24 hours, the prognosis is favorable.
Single dose of Fluoride in unexposed animal
0.06 % in blood Teeth
Soft tissue
After 3 hours
Single dose of Fluoride in continuously exposed animal
( 5 5 days)
After 2 4 hours
F I G . 1 . Distribution of soluble fluoride.
Tissue Analyses
In only a few instances following fatal poisoning by fluoride have tissues removed at autopsy examination been analyzed for the fluoride
content. In various tissues from five such cases Gettler and Ellerbrook (1939) found fluoride contents from 1.6 ppm for brain to 15.6 ppm for lung. Steenhauer and Kedde (1947) gave comparable values for tissues removed from an individual fatally poisoned with sodium fluorosilicate.
The individual data are listed in Table IVA. Fluoride concentrations obtained by Smith et al. (1960 b) in normal tissues are listed in Table IVB.
T A B L E IVA
FLUORIDE CONTENT OF HUMAN TISSUES TAKEN AT AUTOPSY (PARTS PER M I L L I O N OF FLUORIDE)*1
Normal Death from Death from
Tissue deaths5 sodium fluoride6 sodium fluorosilicate0
Blood 0.20-0.64 (4) 3.5-15.5 (5) 5.8 (1)
Brain 0.40-0.68 (4) 1.6-3.4 (2) —
Heart 0.44-0.60 (2) 10.6 (1) —
Kidney 0.56-0.78 (2) 4.6-11.6 (3) —
Liver 0.36-0.70 (3) 4.4-12.2 (5) 7.2(1)
Lung 0.16-0.42 (3) 12.4 -15.6 (2) —
Spleen 0.25-0.30 (2) 11.8 (1) —
Urine 0.40-0.56 (4) — 68.8 (1)
Stomach contents — — 4.4 (1)
Small intestine — — 10.6(1)
contents (in feces)
a Figures in parentheses indicate number of cases.
b Gettler and Ellerbrook (1939).
c Steenhauer and Kedde (1947).
Steenhauer and Kedde's data indicate a rapid removal of fluoride from the stomach into the small intestine and into the urine. Unfortunately, no data are available on the fluoride content of bone specimens from such cases. The bone content should be a more reliable index of the absorbed dose than is the soft tissue content.
Through the courtesy of the late Dr. Thomas A. Gonzales, Chief Medical Examiner for the City of New York, and Mrs. Billie Weil of that office, autopsy records were made available of 119 cases of fatal fluoride intoxication during the interval 1935-1949 (Table III). Analyses for fluoride were performed by Gettler on various organs from 95 cases;
fluoride was found in 82 cases, but was not detected in 13. In Table V, the fluoride concentrations are listed ; the liver and stomach contents were
most frequently analyzed. The fluoride concentrations in the liver range from 1 to 23 ppm with an average concentration of 11 ppm. Quantitative data were reported far less frequently for the stomach contents; fluoride
T A B L E I V B
CONCENTRATIONS OF FLUORIDE IN HUMAN SOFT TISSUES. NORMAL DEATHS (PARTS PER M I L L I O N OF FLUORIDE IN W E T TISSUE)"-6
F(ppm) in
water supply Heart Liver Lung Kidney Spleen Aorta
0.0 (7) 0.64 0.64 0.81 0.63 0.71 8.97
0.0 (7)
0.32-1.25 0.29-1.02 — 0.30-1.02 0.33-1.19 0.79-43.0
1.0 (4) 0.55 0.70 1.20 0.75 0.51 37.9
0.43-0.68 0.27-0.92 0.58-1.81 0.63-0.93 0.55-0.47 11.6-65.7
2.6 (5) 0.67 0.52 1.40 1.32 0.82 14.2
0.37-0.96 0.38-0.73 0.89-2.22 0.54-2.17 0.47-1.19 2.26-21.5
3.7 (4) 0.61 0.60 0.71 0.80 0.68 2.13
0.46-0.88 0.3-1.13 0.54-0.87 0.44-1.48 0.31-1.05 1.41-3.01
4.0 (3) 1.29 0.92 1.98 2.55 — 16.3
0.71-2.14 0.59-1.47 1.06-2.91 0.63-5.45 3.57-22.9
« F. A. Smith et al (1960 b).
b Figures in parentheses indicate number of samples.
was present in from traces to large amounts. The data of Table V are summarized in Table VI. The tissue concentrations in the six instances analyzed in greater detail are in good agreement with those cited previously by Gettler and Ellerbrook.
NONFATAL H U M A N POISONINGS
Roholm (1937 a) compiled the available data (1873-1935) for 13 in
stances involving 51 individuals of acute, nonfatal fluoride poisoning.
As in fatal poisoning, nausea, vomiting, and diarrhea occurred commonly, and there were often abdominal pains and/or cramplike pains in the extre
mities.
During the 62-year interval covered in Roholm's tabulation (1937 a), accidental nonfatal poisonings occurred approximately once in 5 years, whereas during the past 23 years, 20 such poisonings occurred involving at least 576 individuals.
T A B L E V
FLUORIDE CONTENT OF TISSUES TAKEN AT AUTOPSY OF ACUTE, FATAL INTOXICATIONS, N E W YORK C I T Y , 1935-1949»
Stomach
Brain Liver Blood Washings Contents
3.4 ppm 4.4 ppm 4.2 ppm Small amt.
_
— 5.6 — — 1452 ppm
— 15.0 — — 200
— 18.5 — — 3070
— 16.0 — — 486
Large amt. Large amt. — — Large amt.
— 13.3 — — Large amt.
— — — — Large amt.
— Present — — Present
— 5.0 — — 45 mg in half
— 11.0 — — 142 mg in total
— 12.0 — — Large amt. (also in urine)
— 8.0 — — Present
— 12.0 — Present (also in aspirated material)
— 14.0 — — Large amt.
— Trace/100 gm — — Absent
— — — — Large amt. (small amt. in urine)
— Large amt. — — Large amt.
— 15.0 — — Small amt.
— 4.0 — — Small amt. /30 ml; small amt. in
urine
— 6.0 8.0 ppm in kidney; large amt. in urine
— 12.0 — — Small amt. large amt. in urine
— 14.0 — — Large amt.
— 16.0 — Small amt. —
— Present — — Present
— 8.0 — — Present
— 12.0 — — Large amt.
— 15.0 — — Large amt.
— 12.0 — — Large amt.
— Trace — Present —
— 9.8 10.4 Present 10.6 ppm in kidney
1.8 4.5 — — 44.8 mg
— — — — Trace
— — — Small amt.
— Very large amt. in vomitus — —
— 6.0 — 82.5 mg in washings and total contents
6.0 8.0 — — —
— 12 14 ppm in kidney — —
Continued on following page
T A B L E V (continued)
FLUORIDE CONTENT OF TISSUES TAKEN AT AUTOPSY OF ACUTE, FATAL INTOXICATIONS, N E W YORK C I T Y , 1 9 3 5 - 1 9 4 9 "
Stomach
Brain Liver Blood Washings Contents
— 1 2 — — Large amt.
— 1 5 — — Fair amt.
— 1 2 — — Present in stomach
— 1 — — Absent from stomach
— 1 6 — — Large amt.
— 1 5 — — Large amt.
— ·— 1 5 ppm in kidney — Large amt.
— 1.5 — Trace —
6.5 9 . 7 — — 1 1 . 0 mg
— 1 1 . 2 — — 2 8 . 6 mg in total
— 2 2 . 8 — — 1 4 . 3 mg in total 4 . 9 6 . 2 — — Large amt. per 1 0 ml.
— 1 8 — — 2 5 0
— 3 . 5 3 . 0 ppm in kidney — 4 3 0
— 8 . 0 9 . 0 ppm in kidney — 4 8 . 5 mg in half of total
— 8 . 0 — — 5 4 0 mg
— 8 . 0 — Small amt. —
— 4 . 0 Large amt. in 3 0 gm — Trace in 2 0 ml vomitus
— 1 6 . 0 2 2 0 ppm in urine — Small amt.
— 1 6 . 0 — — 5 2 0
— 1 5 . 0 Fairly large amt. — Absent in urine
— 8 . 0 — — Small amt.
— 1 3 . 0 — — Large amt.
— Present — — — 6.5 4 . 5 — — Large amt.
— 1 1 . 0 — — 1 8 4 mg in total 6.0 8 . 0 — — 2 1 5 mg in total
— 1 2 . 0 — Fair amt. Present
— 6 . 0 — — Small amt. in stomach
— 4 . 0 — — —
— 1 8 . 0 — — Present in stomach
— — — — 8 8 0 0 (dose ca. 1 4 gm roach powder)
— 5 . 0 8 ppm in kidney — —
— 1 2 . 0 — — 3 6 0
— — — — Present in large amt.
— 1 2 . 0 — — 3 5 0 0
Continued on following page
T A B L E V (continued)
FLUORIDE CONTENT OF TISSUES TAKEN AT AUTOPSY OF ACUTE, FATAL INTOXICATIONS, N E W YORK CITY, 1 9 3 5 — 1 9 4 9A
Brain
Stomach
Liver Blood Washings Contents
— 1 8 . 0 — —
— Large amt. — —
— 1 5 . 0 — — Composite sample, liver, kidney, blood 8 ppm
— 1 2 . 0 — —
— 1 6 . 0 — —
— Present liver, kidney —
— 1 2 . 0 — — Large amt.
Large amt.
Present in large amt.
Present small amt.
Large amt.
Large amt.
Small amt.
Trace in 1 0 ml
α Unpublished data ( 1 9 5 1 ) from Dr. Thomas A. Gonzales, Chief Medical Examiner, City of New York. Analyses by A. O. Gettler.
T A B L E V I
DISTRIBUTION OF FLUORIDE IN TISSUES FROM CASES OF FATAL SODIUM FLUORIDE INTOXICATIONS, N E W YORK CITY, 1 9 3 5 - 1 9 4 9
Tissue
No. cases analyzed
Range of fluoride content in ppm
Average fluoride content in ppm
Liver Brain Blood
Stomach contents Stomach washings Kidney
Urine
6 4 1 . 0 - 2 2 . 8 7 1 . 8 - 6 . 5 2 4 . 2 - 1 0 . 4 6 6 Trace-large amt.
8 Trace present-small amt.
7 3 - 1 5 7 Small-large amt.
1 0 . 9 5 . 0 7.3
9 . 7
In Table VII are listed the nonfatal poisonings reported since 1935.
Toxic Dose
Serious illness can follow the ingestion of as little as 66 mg of F (146 mg NaF). As with Roholm's tabulation, the actual dose in many cases
TABLE VII ACUTE, NONFATAL FLUORIDE INTOXICATIONS, 1935-1957 Year Investigator Cause Number Fluoride poisoned Preparation compound Dose Symptoms Course 1932 Pigulla (1936 a) Accident Several Insecticide Sodium silico fluoride
Headache, nausea, dizziness, exhaustion, irritability of digestive tract, abdominal colic, sudden attacks of perspiration, increased salivation, piercing chest pains 1936 R. D. Bell (1936) Accident Mixture of Sodium 5.5 grain Vomiting, diarrhea in 10-15 sodium fluoride (358 mg) min. Tingling pains in fluoride extremities, working up- and wards. When seen after 3 sulfur in hr, showed extreme cyan- treacle osis, impalpable pulse. Discharged hospital 4th day
About 14 days 1936 Geiger (1936) Accident 18 Mixture sodium fluoride, bicarbo nate, sold as soda
Sodium Max. dose Vomiting, cramps, diarrhea — fluoride 1 tsp. reported in 8 cases using (5 gm?) mixture in preparation pancakes