PR
Con Offi Hea Mem
REVEN
nsultant: A icial review ad of the F
mbers of th
NTION
Docto
Attila Szab wers: Atti Balá inal Exam
Zolt he Final E
Fere Zsol
N OF AC I
P
Raine
oral Scho Semme
ó, M.D., D ila Tordai ázs Antus mination C án Szabol Examinatio enc Rényi-
lt Csapó M
Bud
CUTE R INJURY
PhD thesi
er Ober
ool of Cli elweis Un
DSc.
M.D., DS MD., DSc Committee
lcs M.D., P on Comm -Vámos M M.D., Ph.D
dapest, 2
RENAL Y
is
rbauer
nical Me niversity
Sc.
c.
e:
Ph.D.
mittee:
M.D., Ph.D D.
2016
L ALLO
edicine
D.
OGRAF FT
1
Table of Contents
The list of abbreviations ... 3
1 Introduction ... 5
1.1 Background and significance ... 8
1.1.1 Delayed Graft Function ... 8
1.1.2 Experimental ARF ... 10
1.1.3 Donor Factors ... 11
1.1.4 Recipient Factors ... 13
1.2 Related Work of other Investigators ... 14
2 Objectives ...16
2.1 Work plan ... 17
3 Methods ...19
3.1 Histogenomics ... 19
3.2 Systems Biology ... 21
3.3 Discovery and Validation Studies ... 23
4 Results ...24
4.1 ARF Specific Molecular Network ... 24
4.2 The Inflammatory Response ... 25
4.3 The RCT – a Logistic Challenge ... 27
4.4 Results on DGF in the RCT ... 32
4.5 Effect of Steroid Donor Treatment on other Transplanted Organs ... 36
4.6 The miRNA Discoveries ... 36
2
4.7 miRNA Target Prediction ... 40
4.8 In vivo Kinetics and Efficacy of Antisense Oligonucleotides ... 43
4.9 Clinical Applicability and Utility ... 45
4.9.1 In vitro Data ... 45
4.9.2 In vivo data ... 47
4.9.3 Abundance of miR-182 target proteins in injured kidneys ... 54
5 Discussion ...60
5.1 Further Work ... 62
6 Conclusions ...63
7 Summary ...64
8 Bibliography ...66
9 Bibliography of the candidate´s publications ...69
10 Acknowledgements ...71
3
The list of abbreviations
DGF delayed graft function DSA donor specific antibodies
ARF acute renal failure
ICU intensive care unit
OR odds ratio
MI myocardial infarction
ReOp reoperation BUN blood urea nitrogen DOI distant organ injury GFR glomerular filtration rate
CFR chronic renal failure
ADH antidiuretic hormone
RCT randomized controlled trial
LCM laser capture microdissection
QC quality control
OEDTR Österreichisches dialysis and transplant registry
POC proof of concept
BCAR biopsy confirmed acute rejection GEO gene expression omnibus
SNPs single nucleotide polymorphism
SIRS systemic inflammatory response syndrome ITT Intention to treat (analysis)
4
ET Eurotransplant SAM significance analysis of microarrays FDR false discovery rate
NaPi2a natrium(sodium) phosphate cotransporter HRPTEC human renal proximal tubule epithelial cells MM mismatch
ASO antisense oligonucleotide
IRI ischemia reperfusion injury PCR polymerase chain reaction HCV hepatitis C virus
5
1 Introduction
Kidney transplantation is clearly the preferred treatment of end stage kidney disease since it allows for a nearly normal life quality and is in the long run considerably cheaper than maintenance dialysis (24).
The incidence rates of patients undergoing kidney transplantation vary considerably among countries and regions reflecting different national regulations and public opinion on organ donation and transplantation in general. The incidence as well as the prevalence of kidney transplantations per million population is in strong correlation with the socioeconomic situation and the Human Development Index (HDI) and income level of countries. Industrialized regions in the world such as USA, Australia and Europe with high HDIs of well above 0.6 show a high incidence (> 30 per million population) of patients undergoing kidney allografting but with a considerable regional variability.
Accordingly, there is also a marked regional and global disparity in the prevalence of kidney transplant patients. The prevalence rates also correlate tight with the socioeconomic status and range from 50 to 300 per million population where the poorest regions have the lowest rates. In countries with a HDI below 0.3 there is virtually no renal transplantation performed. In addition, sound data in these regions are not available and thus an informed discussion on transplantation in these regions is not possible. Lastly, the medical insurance type, religious believes and philosophy are key determinants for access to transplantation.
Given the expenses of this high-end medical procedure requiring the tight collaboration between specialists from different areas such as surgery, immunology, pathology, radiology, tissue typing, infectious disease and nephrology render it intuitive that only countries with working medical infrastructure can offer such regimen. In addition, usually only patients with medical insurance covering such initially expensive
proce allog affor of th dram have kidne
How one y bette
Figu data
Now dono surgi the
edures can graft need to
rdable to pa ese modern matically. N been achie ey transplan
wever; most year graft fu er pre-transp
ure 1. Ann from the Vi
wadays, mod or HLA ant
ical procedu main achie
undergo t o take life-lo
tients with h n immunosu National and eved over t ntation (25)
of the impr function not plant risk ev
nual attrition ienna Trans
dern transpl tibodies (DS
ure in live d evements i
this form o ong immun
health insur uppressants d internation
the last yea .
rovement th t only due to valuation (fi
n of renal splant Cente
lant medici SAs or don donor transp in mid-term
6 of treatmen nosuppressiv
rance or to v in the mid n nal data un ars in prolo
hat was achi o better imm igure 1).
allografts p er).
ine requires nor specific
plantation, a m graft pa
nt. Lastly, t ve drugs, wh
very wealth ninety eight nambiguous onging patie
ieved can b munosuppre
per period o
s the determ antibodies) appropriate atency, the
the recipien hich are exp hy patients.
ties prolong sly show th ent and gra
e attributed essive drug
of transplan
mination of ), technical postoperati
rate of n
nts of a k pensive and
The introdu ged graft sur hat great su aft survival
d to the incr gs but also d
ntation (per
f preformed l planning o
ive care. De not immed
kidney d only uction rvival uccess after
reased due to
rsonal
anti- of the
espite iately
funct high
The early resol all re (figu
Figu last o survi DGF
This risk f DGF prim week
tioning tran level.
incidence o y clinical co lves after so ecipients of ure 2) (26).
ure 2. The in one and a h ival. The re F/ARF comp
highly pre factor for a F have a mo mary or imm
ks but recen
nsplants from
of post-tran ondition wit
ome days b f deceased d
ncidence ra half decade elative risk pared to prim
valent cond a reduced al ore than dou mediate gra nt data sugg
m deceased
splantation th the strong but delayed
donor transp
ates of ARF e remained of graft lo mary functi
dition in de lograft surv ubled risk fo ft function gest that the
7 d organ don
acute rena gest negativ
allograft fu plants but v
F/DGF in th stable at 2 oss more th ioning graft
eceased don vival. Studie or graft loss
(1, 27). D ese allograf
ors remaine
l failure (A ve impact o unction (DG virtually nev
he applicant 25% with a
han doubled ts (PF).
nor transpla es showed t s compared DGF eventu fts are prone
ed unchange
ARF) is the on survival.
GF) affects ver in live d
’s home ins strong asso d in those
ntation repr that kidney to matched ally resolve e to a more
ed at a relat
leading sin ARF event roughly 25 donor transp
stitution ove ociation of transplants
resents the y transplants d transplants es over the e accelerated
tively
ngular tually 5% of plants
er the f graft with
main s with s with e first
d rate
8
of fibrosis, specifically under the current standard immunosuppression of cyclosporine or tacrolimus. These facts clearly show that there is an urgent need for improvement.
1.1 Background and significance
1.1.1 Delayed Graft Function
DGF has been identified as the key target for intervention and great efforts have been undertaken to study the underlying pathophysiology and identify risk factors for ARF as main cause of DGF. There is no uniform definition of post-transplant DGF but most authors use the need of post-transplant dialysis as dichotomous outcome. However, on a more fine-granular basis, DGF/ARF is actually a continuum which ranges from one post-transplant dialysis due to volume management or hyperkalemia to the most extreme other end of the spectrum called primary non-function. The rate of slow or incomplete function is clearly associated with reduced long term patency of the graft and mortality. Longer DGF is also associated with a more pronounced immune response and inflammation in the grafts as evidenced by studies that utilized early protocol biopsies. It is still unclear whether treatment of these early inflammation in these management biopsies with high doses of corticosteroids for example will lead to less fibrosis in the long run and increased graft longevity. Therefore it is of utmost importance to study the signal cascade of DGF/ARF on a molecular level.
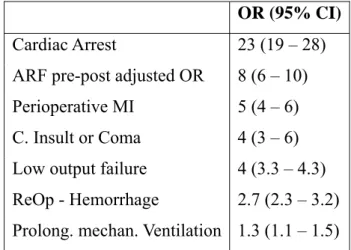
It is likely that post-transplant ARF shares some common features of ARF in the native kidney occurring in roughly one out of four to six patients admitted to the medical ICU (2). If the ARF is so severe that a form of renal replacement therapy is required such as hemofiltration or hemodialysis, the risk of mortality increases dramatically. Studies in patients after cardiac surgery for example showed, that ARF is the second strongest predictor of death after cardiac arrest and ranks even before such devastating conditions as perioperative myocardial infraction or prolonged mechanical ventilation (3) (table 1).
9
Table 1. Risk of mortality expressed as odds ratio (OR) in patients after cardiac surgery developing dialysis dependent ARF compared to equally sick patients without ARF (adapted from Chertow GM et al. (3)).
These results seem initially not intuitive given the fact that renal failure can be treated by hemofiltration, a rather routinely used technique without procedural risk. So why is the risk of dying still so high in patients with ARF?
The likely explanation is that hemofiltration can be used efficiently to remove fluid and low molecular weight ‘toxins’ such as the renal markers creatinine or BUN but cannot normalize the many other malfunctions that are associated and/or caused by ARF. These adverse entities have been recently coined as ‘distant organ injury’ or DOI (4). DOI includes cardiac problems (high output failure, cardiomyopathy, pericarditis), pulmonary comorbidities (edema, alveolitis, pneumonia, hemorrhage), gastrointestinal disease (erosions, ulcerations, hemorrhage, pancreatitis, colitis), neuromuscular pathologies (neuropathy, myopathy, encephalopathy), hematologic/immunologic deficiencies (anemia, thrombopathy, hemorrhage and impaired humoral and cellular host defense) and protein catabolism.
These simple epidemiological analyses which highlight the devastating and essentially poorly treatable condition of the ARF syndrome makes it intuitively clear that prevention of ARF of native kidneys in the ICU and after transplantation is of paramount importance. In order to prevent this condition more insight is required from the initiating and early processes of developing ARF up to the full blown and eventually
OR (95% CI) Cardiac Arrest 23 (19 – 28) ARF pre-post adjusted OR 8 (6 – 10) Perioperative MI 5 (4 – 6) C. Insult or Coma 4 (3 – 6) Low output failure 4 (3.3 – 4.3) ReOp - Hemorrhage 2.7 (2.3 – 3.2) Prolong. mechan. Ventilation 1.3 (1.1 – 1.5)
10
resolving ARF. Since it is not possible to perform sequential renal biopsies on a daily basis experimental animal studies have been used to study postischemic ARF.
1.1.2 Experimental ARF
One of the most representative experimental models for the human situation is the unilateral nephrectomy and clamping of the contralateral renal vascular pedicles in rats for 40 minutes at normothermia. Dialysis dependent ARF in humans is usually multifactorial and occurs predominantly in kidneys with some form of pathology such as atherosclerosis and reduced GFR. Therefore the single kidney ARF of the rat clamp model is also very representative for the human renal allograft setting.
Within one hour after reperfusion the tubular epithelial cell lining is already damaged and one or the other cell became detached from the basement membrane, the tubules are dilated and the creatinine increased twofold (figure 3). One day after reperfusion a full blown ARF developed on a morphological as well as functional level. Most of the tubuli are filled with detritus and fibrin; epithelial cells are predominantly necrotic as evidenced by pycnotic nuclei, and some apoptotic cells. No open lumen is visible within the tubular cross sections and the serum creatinine increased tenfold.
One week after reperfusion the creatinine has returned to normal but the morphology is by far not normal suggesting that creatinine is not a good kidney injury marker because it underestimates the severity of damage dramatically. Morphology improves over time but the late consequences of the ARF are cystic dilatation of some tubuli and higher propensity of chronic renal failure (CRF) as also overserved in patients with initially resolved ICU-ARF. Reemphasizing again however that no morphological data in humans exist because sequential biopsies are not feasible.
Figu Time magn reper arrow nucle the conc morp towa of re Cysti
Drill a mo This trans 1.1.3 The accom cellu dama
ure 3. Morp e on the x-a nification 4 rfusion, tub w). One day ei are pykno
remaining entration h phology is ards its base enal injury.
ic dilated tu
ling from th olecular leve
is especial splant ARF
Donor Fa allogenic t mpanied w ular alteratio
age by reac
phology of d axis refer to
00x, adapte bular dilatio y after reper otic and adj tubule lum has increas
still severe eline value s The late co ubuli are ma
he morpholo el shows sur lly true in
studies.
actors transplantat
ith a period ons of the ti ctive oxygen
developing o 1hour, 1 d ed from Hau on can be s rfusion all a jacent to the men (green sed to its ely impaire suggesting t onsequences aking up mo
ogical level rprising som
the reparat
ion of orga d of hypoxi
ssue of the n species, n
11 ARF in a r day, 1 week user P, Obe seen with o avital cell h
e cell memb n arrow).
maximum ed but the that it is not s of ARF ca ost of the re
deeper into me choreog tion phase
ans from o a over hour donor orga nitric oxide
rat kidney i k and 20 we erbauer R (2 occasional have been sh
brane. Fibri At this st of 3.5mg serum crea t a good bio an be seen a enal parench
o the events raphed proc
of ARF as
one to anot rs leading t n. These ch or peroxini
schemia rep eeks after re 28)). Alread
loss of epi hedded into inous detrit tage the s g/dl. After
atinine has omarker to a at 20 weeks hyma (blue
and process cesses in the s has been
ther organis o a series o hanges main itrite as one
perfusion m eperfusion dy one hour
ithelia cells o the lumen tus is obstru serum creat one week almost retu assess the d s after the i
arrow).
ses that occ e ongoing c shown in
sm is inevi of molecula nly include t e of the stro
model.
(print r after s (red n. Cell
uction tinine k, the
urned degree nsult.
cur on chaos.
post-
itably ar and tissue ongest
12
oxidants that develop in response to hypoxia (5). In addition, a considerable share of the injury observed in the deceased donor kidney is derived from processes occurring in the brain dead donor.
Brain death induces an autonomous storm of cytokines and catecholamines which trigger inflammation followed by profound hypotension after an initial hypertensive crisis and subsequent tissue hypoxemia. This event is perpetuated by the absence of ADH release from the death brain and culminated in the kidneys inability to reabsorb the huge amounts of filtered water eventually culminating in full blown diabetes insipidus. Reactive renal vasoconstriction perpetuates the ischemia/hypoxia of renal tubule epithelial cells as the main target of injury. White and colleagues recently showed that heterotrimeric G-proteins are among the key regulators of renal epithelial cell function during homeostasis and in response to ischemic injury (6). The authors hypothesized that G-protein βγ subunit (Gβγ) dimer activity may be a novel therapeutic target since it is strongly activated during IRI. Eventually, iatrogenic vasopressor use and developing hypernatremia perpetuate these catastrophic processes. A recent study showed that desmopressin use in the donor can ameliorate hyponatremia and was associated with higher propensities of immediate graft function (7).
Ischemic damage of the tissue is further on continued by subsequent reperfusion and flushing with oxygen. Once again, highly reactive and cytotoxic species like the hydroxyl radical lead to further partially irreversible alterations and destruction of the tissue. Even more important, reperfusion of blood into previously damaged tissue is accompanied with a strong immune response resulting in the infiltration of monocytes and neutrophils through the activated endothelium. Taken together, ischemic injury with reperfusion associated inflammatory responses seems to be important factors for the development of ARF.
Additionally, there are certainly post-donor factors such as the duration of cold and likely more important the warm ischemic period that contribute considerably to ARF in
13
the human renal allograft setting. Studies showed that cold static ischemia above twenty hours gradually increase the risk of ARF (27). In recent years machine perfusion techniques have been developed that showed that the risk of ARF, especially in older donors, could be reduced (8). However the reported benefit may even increase by normothermic perfusion of the donor organs (9).
1.1.4 Recipient Factors
Accordingly, the duration of the suture of the vascular anastomosis takes a skilled surgeon in patients with normal anatomy between 30 and 40 minutes. Longer anastomosis times however increase the risk of ARF unproportionally (10). How much the alloimmune response contributes to ARF is not unambiguously determined. Cellular rejection can be clearly differentiated from DGF but the contribution of preformed HLA and non-HLA antibodies is not so easily discernible and no studies investigated morphological and serological features of antibody mediated rejection in first week management or protocol biopsies. However most of the transplant centres nowadays screen patients on the waiting list for the presence of donor specific HLA-antibodies and thus the incidence is likely very low. The contribution of non-HLA antibodies to DGF has not been evaluated yet. In fact there is plausible evidence coming from clinical observations that non-HLA alloimmunity is contributing to ARF/DGF. Patients with Alport syndrome exhibit a full loss of function of the alpha five chain of the type four collagen. If these recipients receive a donor kidney with an intact collagen structure, recipients will make antibodies and a rapid Goodpasture like syndrome develops in roughly 5% leading to early graft loss after prolonged DGF. It is not clear yet why only a minority of cases develop this devastating rapid immune response and why some of the patients develop anti-collagen antibodies but exhibit early and mid-term graft patency. Recent global consortia are currently evaluation the impact of these genetic mismatches between donor and recipient in large genetic associational studies such as the International Genetics & Translational Research in Transplantation Network (www.igenetrain.org).
14 1.2 Related Work of other Investigators
Since ARF/DGF represents one of the main risk factors for premature graft loss and mortality and occurs in roughly one in four transplant recipients, the clinical need for prevention and therapy is evident. Thus many research groups tackled this pathology and investigated adjacent processes from the molecular level up to clinical intervention trials. Recent reviews nicely summarized the current understanding and clinical state of DGF/ARF research and prophylaxis/therapy (11-13, 29).
The transfer of organs from one to another organism inevitably causes some decree of hypoxia which leads to a cascade of molecular and cellular choreographed but also anarchic events and in the donor organ. Ischemic damage of the tissue is aggravated by subsequent reperfusion of the kidney with oxygen containing blood and the alloimmune response of the recipient. Even more important, reperfusion of blood into previously damaged tissue is accompanied with a strong immune response resulting in the infiltration of monocytes and neutrophils through the activated endothelium (30). In summary, ischemic injury with reperfusion associated inflammatory responses seems to be important factors for the development of ARF. There is even evidence that severe brain injury might potentiate the immunologic responses to the graft as a variety of cytokines have been demonstrated to be released in deceased donors (14, 15).
Given the overriding risk of ARF for reduced long-term graft survival and the identified risk factor, several studies investigated preventive measures or strategies. Among the modifiable factors are an optimal donor management and a minimum duration of cold and especially warm ischemic times. Counterbalance of the systemic inflammation of the deceased donor by dopamine has been reported to be associated with a reduced risk of ARF (16). The same authors subsequently showed in a RCT that dopamine donor treatment reduced the need for dialysis after transplantation. However, most of the donors will require vasopressor use anyway and thus we were interested in any additional benefit of an anti-inflammatory intervention. Studies in the late 1970s and early 1980s tackled this enigma but none was randomized and all were of small sample
15
size (17-20). Furthermore, that endpoint was graft loss in this pre-cyclosporine era.
Thus these old studies are not amenable to nowadays clinical practice.
In contrast, three small randomized studies found that corticosteroids plus additional cyclophosphamide in 2 studies did not effect on graft survival within the first year (21- 23). The primary outcome in these trials was short-term graft survival, and their ability to detect important effects of treatment was limited by the low incidence of early graft failure.
The only one adequately powered state RCT on the effect of inhibition of systemic donor inflammation of the incidence and duration of ARF has been conducted by the applicant and will be discussed in detail below (31).
Once ARF has developed in native as well as post-transplant kidneys no causal therapy exists. It is advisable however that those parameters known to contribute to ARF such as arterial hypotension and renal hypoperfusion, infection and inflammation as well as dehydration should be corrected. A scientific proof that these activities actually led to a reduced duration of DGF remains elusive. Nevertheless, the overall ARF rate remains still at a constant high level so that novel approaches for the prevention and treatment of ARF are urgently needed.
16
2 Objectives
The overall aim of this thesis was to elucidate the molecular pathophysiology and discover prognostic factors for posttransplant ARF. The objective was not only to explain the underlying pathophysiology but rather to invent potential preventive and therapeutic strategies to overcome this unwanted phenomenon. By amelioration of the high DGF rates we speculate that the mid- and long term graft survival will increase and shortage of the scare donor organs will be alleviated due to longer lasting grafts. This utilitarian approach has been introduced also in large transplant networks such as in the United States (UNOS) where the donor organ quality is matched with the expected survival of the recipients to avoid futility because currently most of the allograft recipients die with a functioning graft.
In fact based on the findings of our studies a precise goal was to test in vitro and in vivo strategies in experimental models of ARF. Based on these proofs of concept experiments a series of large animal studies will be ultimately performed to test for the applicability of our findings in the setting of human renal transplantation.
Objectives: The molecular regulation of ARF is highly complex and not all parts of the kidney are equally affected. Most of the injury occurs in the tubular epithelial cells and therefore we set out to elucidate the sequential molecular events in microdissected tubules of deceased donor human kidneys. Live donor kidney biopsy specimens were used as healthy controls. Genome wide studies were utilized as tool to derive candidate features of regulation. Since it was expected that several dozens of regulators will be found and that it will be unlikely to find a single therapeutic intervention that captures all of these mediators, miRNA profiles were obtained as well. The specifically designed bioinformatics suite miRway was applied to search for the candidate miRNA that regulated most of these candidates. The causal inference was tested by designing ASOs (antisense oligonucleotides against the target miRNA) to be used for in vivo experiments of ARF.
2.1 A ca half conse overv
Figu trans OED conc
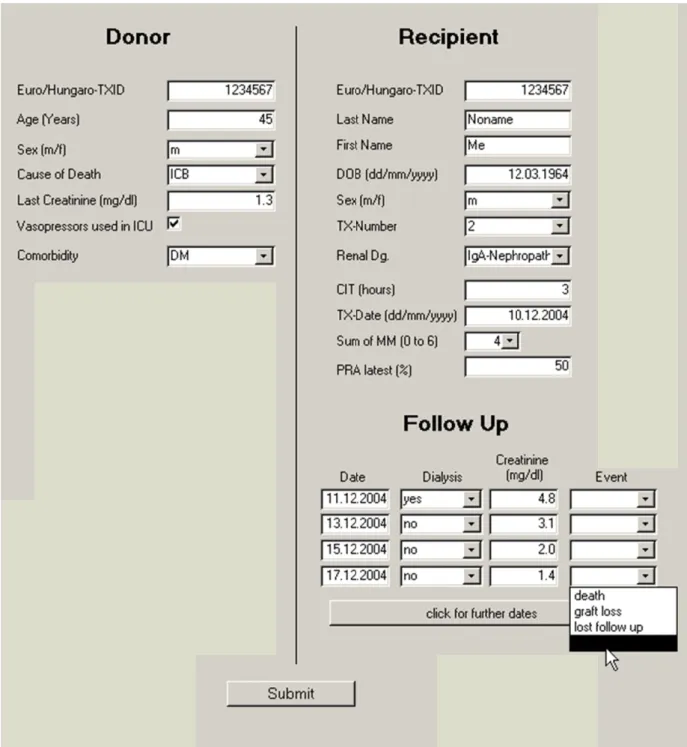
To a decea order rough Semm trans the M to ov recor
Work plan arefully desi
in order t equences a view of this
ure 4. Work splant settin DTR … OE
ept)
assess the ased donor r to have a hly 25%
melweis U splant cente Medical Uni
ver 400 ren rded into a w
n
igned work to thorough and potentia s work plan
k plan for ng (LCM Esterreichis
association kidneys, p a sufficient of decease University C
r roughly 2 iversity of V nal transplan
web-based d
plan has be hly study t al prophyla is illustrate
the study
… laser ca ches Dialy
ns of morp pre-implanta t number o ed donor Clinic in B
00 kidney t Vienna and nts per yea database (fi
17 een set up a the epidem actic and th ed in figure
of ARF ex apture mic yse and Tr
phologic an ation biopsi of outcomes kidney tra Budapest w transplants d the Elisabe
ar. The post igure 5).
and followed miology, pat
herapeutic 4.
xperimentall rodissection ansplant R
nd molecul ies were ob s, i.e. cases ansplants. A was initiate
are perform ethinen hosp t-transplant
d over the l thophysiolo intervention
ly and in t n; QC … Registry; PO
lar features btained in l
s of ARF, A collabor ed since in med annually pital in Linz course was
last decade ogy and cl ns. A sche
the human quality co OC … pro
s in the h large amoun
which occ ration with n this exc
y. Together nz, we had a as monitored
and a inical matic
post- ontrol;
of of
uman nts in cur in h the
ellent r with access d and
Figuure 5. Screennshot of thee web-fronte
18
end of the AARF database
19
3 Methods
A detailed description of all methodological utilized in this research may be found at the applicants website http://www.meduniwien.ac.at/nephrogene under ‘protocols’.
In brief, the following techniques were used in the research projects:
Affymetrix mRNA and miRNA arrays
cDNA Arrays
Cell culture
ELISA
Immunohistochemistry
Peptide Arrays
Protein concentration
qRT - PCR
Western blotting
A detailed description of the animal experiments may be found at the respective sections of this paper.
3.1 Histogenomics
To account for the fact that the kidney does not consist of homogenous tissue but is rather structured into the functional units of nephrons, many of the biopsy specimens obtained were subjected to microdissection. The genome wide gene expression profile was analysed in donor kidney biopsies which developed ARF/DGF after transplantation and compered to signatures in kidneys with primary graft function. The Venn diagram in figure 6 shows the genomic features that discriminated ARF from the primary functioning grafts by tissue compartments.
Figu Abbr glom fibro
The webs
Since given ARF clear
ure 6. Histo reviations r merulosclero
osis, ta … tu
detailed pr site http://ww
e most of t n the highl F, we used a
r results of t
ogenomics o refer to h osis, as … a ubular atrop
rotocol of k ww.meduniw
the gene ex ly complex
an integrati these part of
of donor ki istological arterioloscle
hy, ii … int
kidney gene wien.ac.at/nep
xpression pr changes d ive analytic f the studies
20 idneys (n=8
findings i erosis, ati … terstitial inf
e expression phrogene/ind
rofiles follo during initia cal approach
s.
82) (adapted in the kidn
… acute tub flammation.
n profiling dex.php/prot
ow a highly ation, estab h to derive
d from Perc ney compa ular injury,
may be fo tocol/whole-g
y choreogra blishment an
a sound un
co P et al.
artments: g , if … inter
ound on my genome-arra
aphed patte nd resolutio nderstanding
(32)).
gs … rstitial
y lab- ays-2
er and on of g and
3.2 The colla Emer betw litera
Figu 13,00 biolo
Systems B integrative aboration wi rgentec has ween protein
ature that m
ure 7. Integ 00 vertices ogical data (
Biology e analyses
ith Bernd M s developed n coding f mirror the ph
grated Anal and 800,00 (33).
using a s Mayer and co
an in silico features der hysiological
lyses of a S 00 edges an
21 systems bi oworkers fr o network o rived from
dependenc
Systems Bi nd allows f
ology appr rom emerge of molecula various om ies (figure 7
iology deriv for the integ
roach was entec (www.
r processes mics tracks 7).
ved omicsN grated analy
carried o .emergenetc.
and interac s and publ
NET that c yses of com
ut in com).
ctions lished
covers mplex
The 8A a
Figu
Figu The and i
donor kidne and 8B).
ure 8A. Sche
ure 8B. Sch ARF specif interpretatio
ey profiles
ematic repr
heme of the fic segment on section.
are superim
esentation o
e disease sp ted network
22 mposed on t
of the molec
pecific segm k is shown
the annotate
cular netwo
mented subg in figures
ed relations
ork ‘omicsN
graphs and 10A and 10
s network (f
NET’
functional 0B of the re
figure
units.
esults
3.3 After biops unco of flo obtai in the BAC
Figu expre Indep in sil
Discovery r the transci sies in a n over the com
ow chart is in roughly t e first week CR were tak
ure 9. Wor ession in th pendent val lico analysis
y and Valida iptomics stu novel prosp
mplex mole s depicted i
the same re k and a half ken in the sa
rk flow of he same bi lidation of o s and statist
ation Studie udies, cDNA ective coho cular regula in figure 9.
epresentative after transp ame period a
f the simul opsies in a observed fin tical testing
23 es
A and miRN ort of rena ation of AR . The samp e numbers plantation. T
and served
ltaneous de a prospectiv ndings in th compared t
NA arrays w l allograft RF in furthe ple size of 1
of ARF and Ten protoco
as control ti
etermination ve cohort o
he discover to public do
were conduc recipients w r depth. A 122 donors d BCAR fo ol biopsies w
issue.
n of mRN f renal allo ry cohort w omain data (
cted on the with the ai CONSORT s were chos ollow up bio without ARF
NA and mi ograft recip was performe
(GEO).
same im to T type
sen to opsies F and
iRNA pients.
ed by
4.1 Base defin signi figur the trans
Figu
4 R
ARF Spec ed on the a ned and su
ificant featu re 10B. Mo
gene onto scription fac
ure 10A. AR
Results
cific Molecu available om ubsequently ures and de st of the di logies of ctors.
RF specific
ular Netwo mics profil y superimp ependencies fferentially inflammati
molecular n
24 rk
les (figure posed on t s/interaction y regulated f ion, immun
network of t
10A), an A the omicsN ns between
features in nity and h
the various
ARF specif NET and s the nodes the ARF ki host defen
omics categ
fic network segmented.
are display idneys belo nce, some
gories
k was The yed in ong to were
Figu post- featu
4.2 The i the k well such to ar inflam expre endo repre that kidne
ure 10B. In -transplant ures (34).
The Inflam interpretatio kidneys occu to the abov as the syst rterial hypo
mmation ca ession of pr othelial adh esentants IC subsequent eys that exh
nflammation ARF. The
mmatory R on of the tra urs in the d ve describe emic inflam otension, di
an not only roteins that hesion mol CAM-1, VC tly develop hibited subs
n network i colour cod
Response ansciptomic deceased don
d events th mmatory res iabetes insi y be seen o t are the ma
ecules. Imm CAM-1 and
ed post-tra equently im
25 in donor ki de refers to
cs findings nor before t hat occur du sponse synd ipidus and on the RNA ain effector
munohistoc ELAM-1 sh ansplant AR mmediate gr
idneys whi the gene o
is unambigu the organs a uring the st drome (SIR vasopresso A level but s of the inf chemical st howed a str RF but was raft function
ch subsequ ontologies o
uously that are harveste ay of the d S), renal hy or use. The t is also tra flammation
taining of ong signal i s virtually n (figure 11)
uently deve of the indiv
inflammati ed. This fits donor in the ypoperfusio e observed ranscribed i
cascade su the three in donor kid
absent in d ).
loped vidual
ion in s very e ICU n due renal in the uch as main dneys donor
Figu expre but a pane that mole nece was d
The howe assoc thus cond reduc was d
ure 11. In essed in kid are not det ls). (adapte systemic in ecules in th ssary causa designed an
observed i ever were d ciational fin can only b ducted a RC ction of the defined as t
nflammatory dneys with
tectable in d from Sch nflammation he donor ki ally related
nd conducte
inflammator derived from nding. The be conducte CT to test w e incidence the need for
y proteins subsequent
kidneys w hwarz et al ( n in the bra idneys. It i
to the subse ed (see figur
ry signals m observati
proof of c ed in an in whether the of post-tra r more than
26 (adhesion developme with subsequ
(30)). These ain death d is of notice equent risk re 9 in the n
in the don ional studie ausality of nterventiona treatment o ansplant AR n one post-tr
molecules ent of post-t
uent primar e immunohi donor cause e that the o
of ARF an next paragra
nor kidneys es and thus inflammati al study. T of inflamm RF/DGF. DG
ransplant di
s) are hig transplant A ry allograft istochemica es upregulat observed as nd thus the s aph on RCT
with post- can only b ion as deter herefore, w ation in the GF is the p ialysis. A fi
ghly abund ARF (left pa ft function
al stainings tion of adh ssociation i subsequent T).
t-transplant be consider rminant of we designed e donor cau primary end iner resoluti
dantly anels) (right show hesion is not
RCT
ARF red as ARF d and uses a dpoint ion of
27
the potential effect was the duration of DGF and the number of dialysis session required.
4.3 The RCT – a Logistic Challenge
In this blinded multicentre trial 207 deceased donors were randomized to 1000mg of methylprednislon or placebo single shot injection three to six hours before the organ retrieval. Preimplantation biopsies were obtained to test whether the randomization, timing and dose of the intervention (1000mg methylprednislon) was appropriately chosen to reduce the inflammation cascade on a genome wide level in the kidneys. The biopsies were subjected to microarray testing and the post-transplant course was monitored. A web base case record form (CRF) was used to facilitate the administration of the study and allow for a state of the art online monitoring of the participating centers.
The trial was quite challenging since it is unforeseen where a potential donor will become available and if one is registered, the blinded study medication needed to be carried by the transplant coordinator to the donor site and the verum/placebo injected in the predefined time frame before organ harvest.
The ethical committees of the Medical University of Vienna as well as Eurotransplant approved the study (Ethical Committee of the Medical University of Vienna, Vienna, Austria [study protocol EK-067/2005; to be found at http://ohrp.cit.nih.gov/search]) and the Eurotransplant kidney advisory committee (study protocol 6021KAC06)). A more in depth presentation of the methods and details about the study protocol may be found in the methods section of the publication.
The DGF calcu
Figu dono comp size f an LFU
trial was p F from a hi ulation in th
ure 12. Pow or kidney tr puted samp for 8% lost ITT an U/NU)2=176
powered to istorical 25 he screensho
wer calculat ransplantati ple size to h to follow u nalysis in 6(1/.92)2=20
detect a 50 5% of all d
ot of figure
tion of the ion. Event half event ra up and non-t ncreased
07]
28 0% reductio deceased do
12).
RCT on t rate in the ate was 176 transplanted the samp
on in the i onor transp
he preventi e control g 6. The adju
d (NU … no ple size
ncidence o lants to 12
ion of DGF group was
stment of th on-used) or
to 207
f post-trans 2.5% (see p
F after dec set at 24%
he donor sa rgan plannin 7 [N*=N
splant power
eased
%, the ample ng for N(1/1-
The prede partic the c
Figu al. (3
Detai
number of efined excl cipating ce conducted st
ure 13. CON 31)).
ils on the dem
f 207 dono lusion crite enters. The tudy is illus
NSORT flow
mographic p
ors needed eria includi
CONSORT strated in fig
w chart of t
arameters of
29 to be incr ing kidneys T flow cha gure 13.
the steroid
f the study po
reased to 2 s shipped art (http://ww
donor study
opulation is p
274 to acco in the ET ww.consort-s
y (adapted f
provided in t
ount for va region to statement.org
from Kainz
table 2.
arious non- g/) of
z A et
Tablee 2. Demogrraphic characcteristics of d
30
donors and reecipients by treatment asssignment
31
The transcriptomics experiments on randomly selected 20 biopsies, 10 of each intervention group (steroid/placebo) were conducted on cDNA microarrays holding 41,421 features (batch SHEO) from the Stanford University Functional Genomics core facility. Data analysis was performed by unsupervised hierarchical clustering of biopsies by gene expression (figure 14). The y-axis shows the grouped gene signatures by ontologies. The colour code below the x-axis indicated the relative up- (red) or downregulation (green) of features compared to a set of reference transcripts (Agilent).
As clearly indicated, the steroid pre-treatment of the donors led to a reduction of many features of the inflammation cascades (top lines) and activation of metabolism genes (bottom lines). Based on these data we were confident that the coordination, timing, dosing and intervention of this blinded and logistically challenging worked fine.
Figu two indic diffe ampl 4.4 Desp treatm
ure 14. Uns treatment cated on the
rential regu lified RNA
Results on pite the gl
ment, the in
supervised h groups. Th e right side o ulation of fe (Agilent).
n DGF in th obal suppr ncidence of
hierarchical he gene o of the figur features vs a
he RCT ression of
DGF was n
32 l clustering ontologies o re. The colo
a standard
inflammati not different
of biopsies of differen our code at t
Stratagene
ion in the t between g
s by gene e tially regul the bottom s Universal h
donor org roups (table
expression i ulated gene
shows the x human refe
gans by st e 3).
in the s are x-fold erence
teroid
Tabl 25%
dialy
le 3. The in in the pla ysis was not
ncidence of acebo group t different b
post-transp p respective
etween the
33 plant DGF/A
ely. Also th two groups
ARF in the he number s.
steroid grou of required
up was 22%
d post-trans
% and splant
Acco unch
Figu value
ordingly, th hanged after
ure 15. Traj e refers to th
he resolutio r donor stero
jectories of he F-test in
on of DGF oid treatmen
f post-transp the mixed l
34 as indicate nt (figure 15
plant creati linear mode
ed by creat 5).
inine by ran el for longitu
tinine trajec
ndomization udinal data.
ctories rem
n group. T .
mained
The p-
As se graft evalu of inj
Figu rejec The deriv (adap
econdary en t function o uated. Amat jury and gra
ure 16. Kapl ction (log-ra number of ved from lo
pted from A
ndpoint of t of other tra tschek et al aft patency
lan–Meier e ank p = 0.9 f subjects a og-rank test Amatschek A
this labour, ansplant org
. showed th in liver allo
estimates of 6) risks are at risk is p ts. BCAR, A et al. (35)
35 time and co gans of the hat steroid p ografts (figu
f (A) surviv e shown for provided ab biopsy-con )).
ost intensive e enrolled d pre-treatmen ure 16) (35)
val (p = 0.24 r steroid pre bove the x- nfirmed reje
e academic deceased do nt did not re
.
4) and (B) b e-treated liv axis. Given ection; TX,
study, the i onors have educe that d
biopsy confi vers and pla
n p values , transplant
initial been degree
irmed acebo.
were ation.
4.5 Stero Furth peri- betw fores
Figu treatm (from
4.6 Since suffic were respo In or
Effect of S oid pre-trea hermore, th
transplant l ween treatme st plot in fig
ure 17. Inte ment group m Amatsche
The miRN e it became cient to cha e investigate
onsible for i rder to cov
Steroid Don atment did he trajectori
liver injury ent and base gure 17.
eraction an p. No effect ek A et al. (3
NA Discove e clear that t
ange the ear ed assumin initiation an ver a wider
nor Treatm not effect es of the tr y by steroid eline risk fa
nalysis of g t modificati
35)).
ries the suppres rly outcome ng that othe nd maintena range of r
36 ment on othe
t on the i ransaminase d pre-treatm actors, i.e. d
graft loss ion by the s
ssion of infl es ARF/DG er contribut ance of ARF regulatory t
er Transpla incidence o es showed ment. Post h
donor charac
by various steroid inte
lammation i GF after eng tors than in F leading to target pathw
nted Organ of rejection no impact hoc analysi cteristics is
donor cha rvention co
in the donor graftment, n
nflammatio o DGF after ways than s
ns
ns or mort in the degr s of interac
illustrated i
aracteristics ould be obs
r organs wa novel appro on were cau
r transplant steroid treat
tality.
ree of ctions
in the
s and erved
as not aches usally ation.
tment
37
could accomplish, the microRNA (miRNA) expression in the organs at risk of ARF were determined.
MicroRNAs (miRNAs) are a class of small non-coding 18 to 24 nucleotide-long RNAs that have been implicated recently in diverse cellular functions. miRNAs interfere in translation of mRNAs for a wide variety of proteins regulating cell proliferation, cell death, cellular morphogenesis and differentiation. Production and function of miRNAs requires a set of proteins summarized in the term miRNA machinery (figure 18). A recent summary of the genesis of miRNA, their contribution to pathologies in the transplant kidney as well as potential therapeutic applications may be found in the review by J. Wilflingseder et al.
(36).
Figurre 18. Schemme of miRNAA processing
38
g and its effeccts on transcription and trtranslation
The proto adjus The (37).
Figu accor
simultaneou ocol biopsie stment for m
significant
ure 19. Mol rding to the
us analysis es yielded multiple tes features of
lecular featu eir p-value o
of mRNA several fea sting using f both analy
ures discrim of significan
39 and miRN atures that r
the SAM fa ysis in aggr
minating DG nce.
A transcrip remained s false discove
regate form
GF from pri
pts in the A tatistically ery rate <10 m are display
imary graft
ARF compar significant 0% penaliz yed in figu
t kidney bio red to
after ation.
ure 19
opsies
4.7 The p and predi comp indiv miRw http:/
Figu and comm
miRNA T prediction o only few ta iction routi putational vidual adjus
way
//mirway.nep
ure 20. Scre the underly munication)
Target Predi of miRNA t arget protei ines yield algorithm stment of th
is a
phrogene.at/M
eenshot of t ying databa ).
iction targets is cu ins have be rather inho that allows he significa accessible MirWayFron
the miRNA ase (right p
40 urrently mai een experim omogeneou s the integ ance thresho
on ntend/faces/s
A target pred panel) (Ivce
inly based o mentally val us results,
gration of old (figure my tart.xhtml
diction fron evic S, Stü
on computa lidated. Sin we designe all availab 20). This a lab-w
tend MIRW ütz C et al
ational predi nce the ava
ed a web-b ble routines
algorithm c website
WAY (left p l. 2014 per
iction ilable based s and
oined at
panel) rsonal
We i (figu
Figu ARF
identified m ure 21).
ure 21. Stati F vs PF.
miR-182-5p
istically sign
as the best
nificant disc
41 discrimina
criminator m
ator between
mRNA lead
n DGF and
ds of miR-1
primary pa
82-5p targe atency
ets for
Targ prese cycle FOX
Figu cell c as FO
get candidat ented to be e regulators XO3 (figure
ure 22. Netw cycle regula OXO3 were
te proteins involved in s such as P
22).
work regula ators such a e identified
were ident n ARF regu
CNA, cdc2
ation of pre as PCNA, c as candidat
42 tified and s ulation by c 2, cdk4 or c
edicted miR cdc2, cdk4 tes.
showed man cell cycle re
clock and tr
R-182 target or clock an
ny proteins egulation an ranscription
t proteins. S nd transcript
s that have nd repair su n factors su
Several plau tion factors
been uch as uch as
usible s such
Valid and s
Figu (PGF
4.8 In ex admi DNA in th cells
dation of th showed sim
ure 23. Vali F) vs those t
In vivo Ki xperimenta inistered sh A) end up in
e proximal for at least
he array exp milar regulat
idation of m that develop
inetics and l rat studie hort (18-22m
n the kidney tubule epith four days (
periments fo ion (figure 2
miR-182 arr ped acute ki
Efficacy of es we foun mers) and y. Specifica helial cells (figure 24) (
43 for the lead
23).
ray data by idney injury
f Antisense nd longer syntheticall ally, about 5
of the kidn (27).
miRNA-18
qPCR for g y (AKI).
Oligonucle time ago, ly derived 50% of the eys and rem
82 was perf
grafts with p
eotides that most oligonucleo injected do main stable
formed by q
primary fun
of system otides (anti ose is reabso
inside the t qPCR
nction
ically isense orbed ubule
Figu cells
In ur micro and t
This cotra proxi reabs oligo apica reabs
ure 24. Upt four hours
rine, degra oscopic stu thus may be
hypothesis ansporter N imal tubule sorption. W onucleotides
al membran sorption in i
take of the (A) and fou
aded produc dies showed e suitable fo
s was tested NaPi2a. NaP e and is r We showe s was possi ne of the
isolated bru
antisense o ur days (B)
cts appear d that the ol or antisense
d in vivo by Pi-2a was c responsible
d that a ible and cau proximal tu ush border m
44 oligonucleot
respectively
as early a ligonucleot inhibition o
y inhibiting chosen beca for more
specific used a decr
ubule cell membrane v
tides in the y.
as few hour ides are not of target mR
g the mRNA ause this tr
than 90%
inhibition rease in pho
(25). The vesicles is d
e proximal
rs after inj t trapped in RNAs and m
A of the so ransporter i
of the tub of NaPi2a osphate tran kinetics o isplayed in
tubule epit
jection. Ele n endo-lysos miRNAs.
odium-phos is located i ubular phos a by anti nsport acros
f the phos figure 25.
thelial
ectron somes
sphate in the sphate
isense ss the sphate
Figu antis contr from
4.9
4.9.1 Havi oligo and epith
ure 25. Sele ense oligon rols and the m Oberbauer
Clinical A
In vitro D ing identifi onucleotides
efficacy of helial cells (
ective inhibi nucleotides e unaffected r R et al. (38
Applicability
Data
ed miR-18 s (ASO, an f miR-182 (HRPTECs)
ition of the (AS). Rev d sodium su 8)).
y and Utility
2 as candi natgomiRs) inhibition ).
45 renal sodiu ersed seque ulfate transp
ty
idate interv against mi in cell cul
um phospha ences of th porter were
ventional le iR-182 and ture of hum
ate cotransp e AS (rAS) used as ref
ead, we des d evaluated man renal
porter NaPi ) and scram ference (ad
signed anti their selec proximal t
2a by mbled dapted
isense ctivity ubule
Studi
Figu 25mM as w expe
ies showed
ure 26. Anta M antagom well as vehi
riments.
a dose depe
agomiR inh miR-182 (AS
icle and sa
endent inhib
hibition of m SO) blocke
line contro
46 bition of the
miR-182 in ed the targe ol did not a
e target miR
n cultured H t miRNA, m affect miRN
RNA in vitro
HRPTEC in mismatched NA abunda
o (figure 26
n vitro. Dos d controls ( ance in the
6).
ses of (MM) PCR
4.9.2 Acut left r
Figu cross
Rats 25mM expre (figu
In vivo da te renal failu renal artery
ure 27. Rat s clamping o
were pretr M) or equa ession of m ure 28).
ata
ure was ind for 40 minu
model of A of the left re
reated 12 ho al concentra miR-182 re
duced in SD utes (figure
ARF. Anim enal artery f
ours before ations of m mained sel
47 rats by righ
27).
mals were su for 40 minu
e insult with mismatched lectively re
ht uninephr
ubjected to utes.
h either ana antisense duced in th
ectomy and
sided unin
atgomiR-18 oligonucleo he anatagom
d clamping o
nephrectomy
82 (ASO 2.5 otides. Intra
miR treated of the
y and
5 and arenal d rats
Figu reper antis
The injur insul (crea respe
Figu reper equa
ure 28. Intr rfusion. Ra ense 12 hou
trajectories ry. Histolog lt. Antagom atinine and
ectively.
ure 29. Traj rfusion inju al concentrat
rarenal exp ats were p urs before in
s of serum gical evalua miR-182 (A
BUN) and
ajectories of ury in rats.
tions of mis
pression of pretreated w
nduction of
creatinine ation of kid ASO) treatm
morpholog
f serum cre ASO low smatched co
48 miR-182 a with either f injury.
were deter dney was pe
ment led t gical insult
eatinine ove refers to an ontrol.
at various r antagomi
rmined dail erformed on to an amel
as evidenc
er the first n antimiR c
time points iR (ASO)
ly for seven n days two lioration of ce in figure
seven day concentratio
s after isch or misma
n days afte and seven f the funct es 29, 30 an
ys after isch on of 2.5m
hemia atched
er the n after tional nd 31
hemia mM or
Figu injur conc
ure 30. Traj ry in rats.
entrations o
jectories of ASO low of mismatch
f BUN ove refers to hed control.
49 er the first
an antimiR
seven days R concentr
after ische ration of 2
emia reperf 2.5mM or
fusion equal
Figu treate antim phos degre left comp
ure 31. Hist ed as well miR pretrea phatase pro ee of injury lower corn pared to the
tomorpholo as untreate atment as oduction an y. The treat ner. ASO ( e control (pl
ogy of repre ed controls.
indirectly nd thus diff
tment group (lower righ lacebo and A
50 esentative r . Damage c
also evide ferent colou p and time ht) treated ASO-misma
rat kidneys could be dr nce by int ur intensitie after injury rats showe atch) group
of anti-miR ramatically tact brush es are corre y in days is ed dramatic
s.
R and mism y reduced b
border alk esponding t
indicated i cally less i
match by the
kaline to the in the injury
Morp patho evalu histo
Figu after high
phological e ologist. Inju uated kidn opathology s
ure 32. Sem IRI. Anti-m to 25mmol
evaluation o ury severity
eys per g scores are p
miquantiativ miR (ASO) l.
of the vario y was score groups and provided in f
ve scoring o ), MM (mis
51 ous treatme ed semiquan
time afte figure 32.
of the injury smatched A
nt groups w ntitatively f er ischemia
y severity b ASO), low re
was perform from 0 to 3.
a reperfusi
by treatmen efers to a d
med by a bl . The numb ion as we
nt class and dose of 2.5m
inded ber of ell as
d time mmol,
The seven the o (figu
Figu selec ASO discr effica
long-term e n day exper ontologies o ure 33).
ure 33. Unsu cted three A O (antimiR-1
riminate at d acy of ASO
effects of th riments but
of fibrosis
upervised cl ASO and thre
182) treated day two bu O (antimiR-1
he ASO int it is interest were mark
lustering of ee control tr d rats (indic ut already at 182) in fibro
52 tervention c
ting that alr kedly suppr
f gene ontol reated rat k cated as t_) t day seven
osis preven
can certainl ready at sev ressed in A
logies of fib kidneys two ) and placeb
suggesting tion.
y not be ev ven days, ge ASO treated
brosis pathw and seven d bo (indicate g also poten
valuated in enes belongi d rats vs co
ways in rand days after in ed as p_) di ntial of long
these ing to ontrol
domly njury.
id not g term
53
The following 20 genes were selected on the basis of public domain databases such as GEO (table 4).
Table 4. Fibrosis and connective tissue markers represented on the Affymetrix platforms. These ontologies were specifically analysed in order to elucidate whether ASO (antiMir-182) could act on prevention of fibrosis as the long-term consequence of ARF.
Fibrosis marker Collagens
AngII COL4A1 AT1 COL4A2 AT2 COL4A3 AGE COL4A4 RAGE COL4A5 TGFB1 COL4A3bp TGFBR2
TGFBRI IL1B TNFA SMAD2 SMAD3 SMAD4 SMAD7 IKBA P50 P65 ERK P38
4.9.3 Ther treatm figur http:/
and c
Figu (© n
So fa How apop
Abundanc re are likely
ment given re 18). Ou //mirway.nep cell viability
ure 34. miR ephrogene)
far only few wever, many ptosis. Thus
ce of miR-18 y many effec n the fact th ur custom phrogene.at/M
y/apoptosis
R-182 target .
w of the pr y targets b s it is of n
82 target pro ctor protein hat miRNA mir targ MirWayFron regulatory
features pre
redicted targ belong to note that s
54 oteins in injur ns of the obs As regulate a get predicti
ntend/faces/s proteins an
edicted by o
get proteins protein net suppression
red kidneys served effec a whole ne ion tool m
tart.xhtml p nd adjacent p
our custom
s have been tworks of
of miRs t
ct of anatgo twork of pr mirway, to predicted se pathways (f
mirway bio
n experime cell cycle that inhibit
omiR-182 (A roteins (see o be foun everal cell figure 34).
oinformatic
entally valid regulation t cell cycle
ASO) e also nd at
cycle
s tool
dated.
n and e and
antia hypo 48 an were
Figu anti-m injec
apoptosis w othesis, mice
nd 96 hours e performed
ure 35. Bcl- miR-182 (A cted with AS
ould lead to e were injec s respectivel d and the res
-2 and Foxo ASO) versu
SO or place
o a more ef cted with A ly. Western sults are disp
o-1 protein s placebo (M ebo.
55 fficient rege ASO or place n blots of th
played in fi
are activate MM-ASO)
eneration of ebo control he candidate
igure 35.
ed (inhibitio . Experimen
f injured tis and kidney e proteins B
on of inhibit nts were pe
ssue. To tes ys harvested cl.2 and FO
tory miRNA erformed in
st this d after OXO1
A) by mice
56
After investigations from cell culture to whole animal experiments showed that anti- miR-182 selectively inhibited miRNA-182 activity and activation of target proteins as well as amelioration of IRI in the rat models, we proceeded with studies of anti-miR- 182 in ex vivo perfused pig kidneys. Freshly harvested pig kidneys were subjected to ex vivo normotheric machine perfusion with UW solution (University of Wisconsin) solution at a pressure of 80mmHg. The setup of the experiment is illustrated in figure 36.
Figu 80mm
ure 36. Nor mHg.
rmothermicc machine p
57
perfusion oof a pig kidney with UW solutiion at
58 The experimental set up is provided as:
• Run for 6.5 hours
• Antisense oligonucleotide was administered after 30 minutes of perfusion and circulated for 6 hours
• Pressure: 75-90 mmHg (depending on position of the cannulas)
• Flow: 0.14-0.188 L/min (increased in the first 2 hours then remained constant)
• O2 consumption 68% after 30 minutes of perfusion, 48% after 3h of perfusion
• Biopsies were taken regularly (every 2 hours) For RNA extraction
For protein extraction
For histology
• Urine samples were taken regularly
• Urine produced: 20-40ml/30min, increased slowly
Quan miR- deter isola
Figu biops miRN
ntitative PC -182 over t rmined sinc ated perfused
ure 37. Inhi sies of norm NA to test t
CR of the bi the perfusio ce the half-li
d organs lar
ibition kine mothermic e the selectivi
iopsies from on time of
ife of these rgely unkno
etics of miR ex vivo per ity of the an
59 m the pig k
six hours proteins is own.
R-182 by a rfused pig k ntisense con
kidney show (figure 37) considerab
antisense ol kidneys. miR nstruct.
wed a select ). Target pr ly longer an
ligonucleoti R-146b was
tive inhibiti roteins wer nd the kinet
ide in sequ s used as co
ion of re not tics in
ential ontrol