III./4.6. Status epilepticus
Status epilepticus is defined as one continuous unremitting seizure lasting for longer than 30 minutes, or recurrent seizures where consciousness is not regained between seizures for longer than 30 minutes. Recently, it has become clear that this definition of a 30 minute-long period may be too long, and a new guideline is being developed which recommends that seizures lasting longer than 5 minutes should be treated as status epilepticus. Early treatment of seizures is associated with fewer complications and a lower risk of refractory status epilepticus.
Status epilepticus may be generalized or focal, convulsive or
non-convulsive. Electrographic status epilepticus (continuous epileptic activity on the EEG without clinical symptoms) should be considered in the differential diagnosis of conditions causing unconsciousness.
Generalized convulsive status epilepticus may present as generalized tonic-clonic seizures, myoclonic seizures (often in post-hypoxic states), tonic seizures or clonic seizures.
Focal convulsive seizures may present as epilepsia partialis continua (see III.4.3.) or as hemi-convulsion.
A non-convulsive status epilepticus may be an absence status or the generalized electrographic status in unconscious patients mentioned before.
Non-convulsive focal status may be caused by simple partial or complex partial seizures. Focal electrographic status epilepticus may occur in unconscious patients.
Childhood status epilepticus occurs mainly in connection with fever or infections. In adult epileptic patients, the main causes of grand mal status epilepticus include AED withdrawal, acute cerebral embolisation, metabolic disorder or alcohol intoxication. The mortality of status epilepticus is still high. Mortality is reported to be 50-86% in myoclonic status epilepticus, and 30% in grand mal status epilepticus. The risk of fatal outcome is higher in elderly patients and in long lasting status epilepticus.
In clinically obvious cases, medical treatment has to be started
immediately even before the diagnosis of status epilepticus is confirmed by EEG. However, the termination of status epilepticus has to be confirmed by EEG, because non-convulsive or electrographic status epilepticus may continue without clinical symptoms. Non-convulsive epilepsy may be the cause of unexplained behavioral disturbances in 40% of such cases. This ratio is even higher in the group of critically ill patients (e.g. in intensive care units).
EEG in status epilepticus helps in monitoring the effect of AED treatment, and shows the level anesthesia (burst-suppression patterns appears)in patients requiring anesthesia.
Pharmacological treatment has to be started as soon as possible. The risk of a focal status epilepticus turning into a generalized status epilepticus is relatively high; therefore, the treatment is similar in both forms.
The aim of treatment is to stabilize vital functions (respiration and circulation) and to stop the seizures (both clinical and electrographic
seizures).
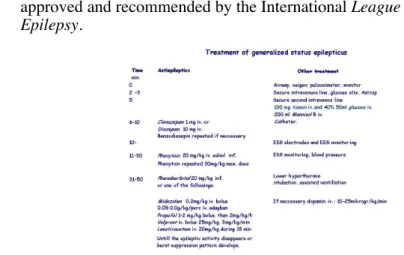
Fig. 9 shows the treatment protocol of status epilepticus in adults approved and recommended by the International League Against Epilepsy.
Fig.9: The treatment protocol of status epilepticus in adults approved and recommended by the International League Against Epilepsy