www.revportcardiol.org
Revista Portuguesa de
Cardiologia
Portuguese Journal of Cardiology
ORIGINAL ARTICLE
Mitral annulus is dilated with preserved function in acromegaly regardless of its activity: Insights from the three-dimensional speckle-tracking echocardiographic MAGYAR-Path Study
Attila Nemes
a,∗, Árpád Kormányos
a, Péter Domsik
a, Anita Kalapos
a, Csaba Lengyel
b, Nóra Ambrus
a, Zsuzsanna Valkusz
ba2ndDepartmentofMedicineandCardiologyCentre,FacultyofMedicine,AlbertSzent-GyörgyiClinicalCenter,Universityof Szeged,Szeged,Hungary
b1stDepartmentofMedicine,FacultyofMedicine,AlbertSzent-GyörgyiClinicalCenter,UniversityofSzeged,Szeged,Hungary
Received21April2020;accepted8July2020 Availableonline1March2021
KEYWORDS Acromegaly;
Mitralannulus;
Three-dimensional;
Echocardiography
Abstract
IntroductionandObjective:Acromegalyisarare,chronicandslowlydevelopingendocrinedis- ordercausedby hypersecretion ofhuman growthhormoneandconsequently ofinsulin-like growthfactor-1duringadulthood.Thepresentstudywasconductedtoassessmitralannular (MA)sizeandfunctionbetween acromegalicpatientsandage-andgender-matchedhealthy controlsby three-dimensional speckle-tracking echocardiography(3D-STE). Italso aimed to examinewhetheractivityofthediseasehasanyeffectonMAparameters.
Methods:Thisstudyincluded27patientswithacromegaly,threeofwhomwereexcludeddue toinferiorimage quality. Themean age oftheremaining24 patients was 55.7±14.0 years andsevenweremale.Completetwo-dimensionalDopplerechocardiographyand3D-STEwere performedinallcases.
Results:Significantlyincreasedend-diastolicandend-systolicMAdiameter(2.81±0.36cmvs.
2.44±0.34cmand2.00±0.32cmvs. 1.65±0.37cm, respectively),area (9.67±2.33cm2vs.
7.38±1.93cm2and5.14±1.62cm2vs.3.74±1.19cm2,respectively)andperimeter(11.76±1.42 cmvs.10.27±1.33cmand8.61±1.23cmvs.7.36±1.10cm,respectively)weredemonstrated inacromegalicpatients comparedwithcontrolsubjects.MAfunctionalparameterswerenot significantlyalteredcomparedtothoseofhealthyindividuals.
∗Correspondingauthor.
E-mailaddress:nemes@in2nd.szote.u-szeged.hu(A.Nemes).
https://doi.org/10.1016/j.repc.2020.07.018
0870-2551/©2021SociedadePortuguesadeCardiologia.PublishedbyElsevierEspa˜na,S.L.U.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Conclusions: MAdilationcouldbeseeninacromegalyregardlessofitsactivity.Acromegalyis notassociatedwithMAfunctionalimpairment.
©2021SociedadePortuguesadeCardiologia.Publishedby ElsevierEspa˜na, S.L.U.Thisisan openaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by- nc-nd/4.0/).
PALAVRAS-CHAVE Acromegalia;
Anelmitral;
Tridimensional;
Ecocardiografia
Dimensõesefunc¸ãodoanelmitralnaacromegalia:dadosdoestudoMAGYAR-Pathpor ecocardiografiatridimensionaldespeckletracking
Resumo
Introduc¸ãoeObjectivo: A acromegalia é uma doenc¸a endócrina rara, crónica e de desen- volvimento lento, causada pela hipersecrec¸ão da hormona do crescimento humano e, consequentemente,dofatordecrescimentosemelhanteàinsulina-1duranteaidadeadulta.
Opresenteestudofoiconduzidopara avaliarotamanhoeafunc¸ãodoanelmitral(MA)nos doentescomacromegaliaecontrolessaudáveisemparelhadosporidadeesexo,pormeiode ecocardiografiatridimensionalcomspeckle-tracking(3DSTE).Oobjetivofoitambémexaminar seaatividadedadoenc¸atemalgumefeitonosparâmetrosdaMA.
Métodos: Este estudo incluiu27 pacientescomacromegalia, três dos quais tiveram deser excluídosdevidoàqualidadeinferiordeimagem.Amédiadeidadedos24pacientesrestantes foide55,7±14,0anos(7homens).Foramrealizadosemtodososcasosumaecocardiografia Dopplerbidimensionalcompletaeum3DSTE.
Resultados: Quando comparados comos controlos, os doentesacromegálicos apresentaram diâmetrosdiastólicoesistólicofinaissignificativamentedilatados(2,81±0,36cmversus2,44
±0,34cme2,00±0,32cmversus1,65±0,37cm,respetivamente),assimcomoaáreavalvular (9,67±2,33cm2versus7,38±1,93cm2e5,14±1,62cm2versus3,74±1,19cm2,respetiva- mente)eoperímetro(11,76±1,42cmversus10,27±1,33cme8,61±1,23cmversus7,36
±1,10cm,respetivamente)OsparâmetrosfuncionaisdaMAnão estavamsignificativamente alteradosemcomparac¸ãocomindivíduossaudáveis.
Conclusões: Adilatac¸ãodoMApodeserobservadanaacromegalia,independentementedesua atividade.AacromegalianãoestáassociadaaocomprometimentofuncionaldaMA.
©2021SociedadePortuguesadeCardiologia.PublicadoporElsevierEspa˜na,S.L.U.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by- nc-nd/4.0/).
Introduction
Acromegaly is a rare, chronic and slowly developing endocrine disorder caused by hypersecretion of human growth hormone (hGH) and consequently of insulin-like growthfactor-1(IGF-1)duringadulthood.1Acromegaliccar- diomyopathy is reportedtobeoneof themost important complicationsofacromegalyandcardiovasculareventsmay belinked tothesehormones.2---4 The saddle-shapedmitral annulus(MA)playsanimportantroleinthefillingandempty- ingoftheleftheartchambers.PerturbationsofMAgeometry andfunctioncanbeseeninanumberofdiseases,particu- larlyinvalvulardisordersandatrial fibrillation.5However, somenon-valvulardisordershavealsobeenfoundtobeasso- ciatedwithMAmorphologicalandfunctionalalterations.6---8 The present study was conducted to compare MA size and functional properties between acromegalic patients and age- and gender-matched healthy controls by three- dimensionalspeckle-trackingechocardiography(3D-STE).
Methods
Patientpopulation
The study included 27 patients withacromegaly, threeof whom were excluded due to inferior image quality. The meanageoftheremaining24patientswas55.7±14.0years andseven weremale. Their resultswere comparedto38 healthycontrols(meanage:53.4±4.4years,16male).For all patients and controls, 3D-STE wasperformed in addi- tiontoroutinetwo-dimensionalDopplerechocardiography.
The diagnosis of acromegaly was based on and its activ- itywas definedin accordance withcurrent guidelines, as detailedpreviously.1Allacromegalicpatientswereincluded in the Motion Analysis of the heart and Great vessels bYthree-dimensionAlspeckle-tRackingechocardiographyin Pathologicalcases (MAGYAR-PathStudy). Allpatients gave their informed consent. The study was approved by the humanresearchcommitteeattheUniversityofSzegedand
254
Figure1 Imagesfromthethree-dimensionalfull-volumedatasetshowingthemitralannulusinapatientwithacromegalyincluding apical4-chamber(A)and4-chamber(B)long-axisviewsandacross-sectionalviewatthelevelofthemitralannulus(C7)optimized inlong-axisviews.Area:mitralannulararea;Circ:mitralannularperimeter;Dist:mitralannulardiameter;LA:leftatrium,LV:left ventricle,RA:rightatrium,RV:rightventricle.
followed theethicalguidelinesofthe 1975Declaration of Helsinki.
Two-dimensionalDopplerechocardiography
A Toshiba ArtidaTM echocardiograph (Toshiba Medical Sys- tems, Tokyo, Japan) with a PST-30SBP phased-array transducer (1-5 MHz) wasused to perform standard two- dimensional (2D) Doppler transthoracicechocardiographic examinationsfollowingrecentguidelines.9Aqualitative(0- 4) scale was usedto grade mitral regurgitation,where 0 representsnoregurgitationand4standsforthemostsevere regurgitationpossible.
Three-dimensionalspeckle-tracking echocardiography
3D-STE was performed with the same Toshiba ArtidaTM echocardiograph (Toshiba Medical Systems, Tokyo, Japan) attachedto a PST-25SX matrix-arraytransducer.10 An api- calwindowwasusedfor3D-STEdataacquisition,inwhich sixwedge-shapedsubvolumeswereacquiredduringasingle breath-holdin sinus rhythm, fromwhich afull-volume3D datasetwascreatedautomatically.Offlineanalysisofthe3D datasetswascarriedoutusing3DWallMotionTrackingsoft- ware,version2.7(ToshibaMedicalSystems,Tokyo,Japan).
Apical2-chamberand4-chamberviewsandthreeshort-axis views---basal(C7),midventricularandapicalleftventricular (LV)levels---wereselectedatend-diastolebythesoftware.
Following optimization of imaging planesin apical 4- and 2-chamberviewsontheedgesoftheMA,severalMAmor-
phologicalparametersweremeasuredin theC7short-axis view. The following morphological parameters were mea- suredatend-diastole(justbeforemitralvalveclosure)and end-systole(justbeforemitralvalveopening)(Figure1)6---8: - MA diameter (MAD), defined as the perpendicular line drawn from thepeak of MA curvature tothe middle of thestraightMAborder(anteroposteriordiameter);
- MAarea(MAA)measuredbyplanimetry;
- MAperimeter(MAP)measuredbyplanimetry.
Usingtheaboveparameters,thefollowingMAfunctional propertieswerecalculated:
- MAfractionalshortening(MAFS),definedas([end-diastolic MAD−end-systolicMAD]/end-diastolicMAD)×100, - MA fractional area change (MAFAC), defined as
([end-diastolic MAA−end-systolic MAA]/end-diastolic MAA)×100.
Statisticalanalysis
Alldatawerepresentedasnumber(percentage)ormean± standarddeviation.Differencesinvalueswereconsideredto bestatisticallysignificantwithp<0.05.Pearson’scoefficient wasusedforcorrelationbetweenvariables.BlandandAlt- man’smethodwasusedforstudyingintra-andinterobserver agreement. Data analyses were performed using RStudio Teamstatisticalsoftware(RStudio:IntegratedDevelopment forR.RStudio,Inc.,Boston,MA,2015).
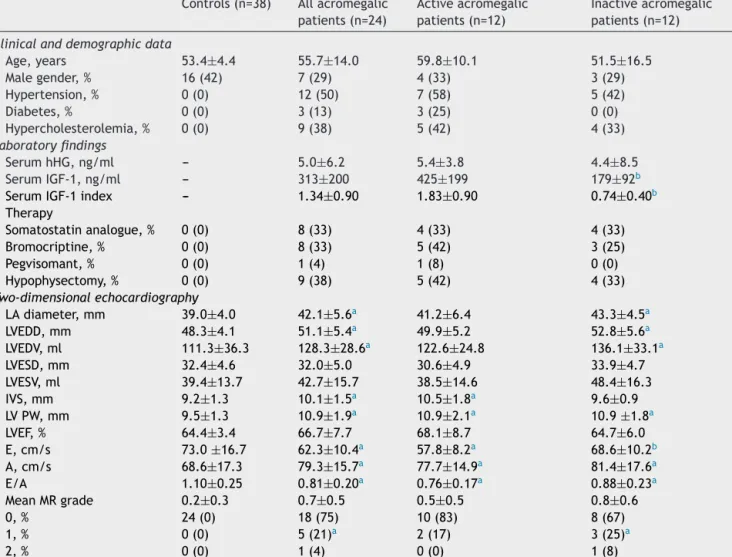
Table1 Clinical,demographicandtwo-dimensionalechocardiographicdatainacromegalicpatientsandmatchedcontrols.
Controls(n=38) Allacromegalic patients(n=24)
Activeacromegalic patients(n=12)
Inactiveacromegalic patients(n=12) Clinicalanddemographicdata
Age,years 53.4±4.4 55.7±14.0 59.8±10.1 51.5±16.5
Malegender,% 16(42) 7(29) 4(33) 3(29)
Hypertension,% 0(0) 12(50) 7(58) 5(42)
Diabetes,% 0(0) 3(13) 3(25) 0(0)
Hypercholesterolemia,% 0(0) 9(38) 5(42) 4(33)
Laboratoryfindings
SerumhHG,ng/ml --- 5.0±6.2 5.4±3.8 4.4±8.5
SerumIGF-1,ng/ml --- 313±200 425±199 179±92b
SerumIGF-1index --- 1.34±0.90 1.83±0.90 0.74±0.40b
Therapy
Somatostatinanalogue,% 0(0) 8(33) 4(33) 4(33)
Bromocriptine,% 0(0) 8(33) 5(42) 3(25)
Pegvisomant,% 0(0) 1(4) 1(8) 0(0)
Hypophysectomy,% 0(0) 9(38) 5(42) 4(33)
Two-dimensionalechocardiography
LAdiameter,mm 39.0±4.0 42.1±5.6a 41.2±6.4 43.3±4.5a
LVEDD,mm 48.3±4.1 51.1±5.4a 49.9±5.2 52.8±5.6a
LVEDV,ml 111.3±36.3 128.3±28.6a 122.6±24.8 136.1±33.1a
LVESD,mm 32.4±4.6 32.0±5.0 30.6±4.9 33.9±4.7
LVESV,ml 39.4±13.7 42.7±15.7 38.5±14.6 48.4±16.3
IVS,mm 9.2±1.3 10.1±1.5a 10.5±1.8a 9.6±0.9
LVPW,mm 9.5±1.3 10.9±1.9a 10.9±2.1a 10.9±1.8a
LVEF,% 64.4±3.4 66.7±7.7 68.1±8.7 64.7±6.0
E,cm/s 73.0±16.7 62.3±10.4a 57.8±8.2a 68.6±10.2b
A,cm/s 68.6±17.3 79.3±15.7a 77.7±14.9a 81.4±17.6a
E/A 1.10±0.25 0.81±0.20a 0.76±0.17a 0.88±0.23a
MeanMRgrade 0.2±0.3 0.7±0.5 0.5±0.5 0.8±0.6
0,% 24(0) 18(75) 10(83) 8(67)
1,% 0(0) 5(21)a 2(17) 3(25)a
2,% 0(0) 1(4) 0(0) 1(8)
E/A:ratioofearlyandlatediastolictransmitralflowvelocity;hGH:humangrowthhormone;IGF-1:insulin-likegrowthfactor-1;IVS:
interventricular septum;LA: leftatrial;LV:left ventricular;LVEDD:end-diastolicdiameter;LVEDV:end-diastolicvolume; LVEF:left ventricularejectionfraction;LVESD:end-systolicdiameter;LVESV:end-systolicvolume;MR:mitralregurgitation;PW:posteriorwall.
a p<0.05vs.controls.
b p<0.05vs.activeacromegalicpatients.
Results
Clinical,laboratory,therapeuticand two-dimensionalechocardiographicdata
Significantdifferencesweredemonstratedinmostechocar- diographicparametersbetweenallacromegalicpatientsand healthy control subjects. Differences between active and inactiveacromegalicpatientsandcontrolsarepresentedin Table1.IGF-1levelsandindicesandearlytransmitralflow velocitydifferedsignificantlybetween activeandinactive acromegalicsubjects(Table1).
Three-dimensionalspeckle-tracking echocardiography-derivedmitralannular parameters
SignificantlyincreasedMAdimensionsweredemonstratedin acromegalicpatients.MAfunctionalpropertiesdidnotdiffer
between patients with acromegaly and age- and gender- matched controls. No differences in MA data were seen accordingtotheactivityofacromegaly(Table2).
Correlations
No significant correlations were detected between MA parametersanddifferenthormonelevels.
Reproducibility measurements
The differences (mean ± standard deviation) measured by two observers for end-diastolic MAD, MAA and MAP were 0.01±0.18 cm, -0.04±0.79 cm2 and ---0.19±0.98 cm, respectively, with correlation coefficients between these independent measurements of 0.97 (p<0.0001), 0.96 (p<0.0001) and 0.97 (p<0.0001), respectively (inter- observer variability) at rest. The corresponding values
Table2 Comparisonofthree-dimensionalspeckle-trackingechocardiography-derivedmitralannularmorphologicalandfunc- tionalparametersbetweenpatientswithacromegalyandcontrols.
Controls(n=38) Allacromegalic patients(n=24)
Activeacromegalic patients(n=12)
Inactiveacromegalic patients(n=12) MAmorphologicalparameters
MAD-D,cm 2.44±0.34 2.81±0.36a 2.86±0.41a 2.76±0.32a
MAA-D,cm2 7.38±1.93 9.67±2.33a 10.12±2.58a 9.22±2.05a
MAP-D,cm 10.27±1.33 11.76±1.42a 11.96±1.59a 11.56±1.27a
MAD-S,cm 1.65±0.37 2.00±0.32a 2.08±0.31a 1.91±0.31a
MAA-S,cm2 3.74±1.19 5.14±1.62a 5.43±1.45a 4.85±1.79a
MAP-S,cm 7.36±1.10 8.61±1.23a 8.87±1.10a 8.35±1.34a
MAfunctionalparameters
MAFAC,% 48.3±16.1 46.4±11.3 45.3±11.3 47.6±11.7
MAFS,% 32.7±13.9 28.6±9.4 26.3±11.3 30.9±6.7
MA:mitralannular;MAA-D:end-diastolicmitralannulararea; MAA-S:end-systolicmitralannular area;MAD-D:end-diastolic mitral annular diameter;MAD-S:end-systolicmitralannulardiameter; MAP-D:end-diastolicmitralannular perimeter;MAP-S:end-systolic mitralannularperimeter;MAFAC:mitralannularfractionalareachange;MAFS:mitralannularfractionalshortening.
a p<0.05vs.controls.
for intraobserver variability including values obtained by two measurements by observer 1 were -0.03±0.19 cm, 0.03±1.04 cm2 and -0.01±0.95 cm, respectively, with correlation coefficients between these independent mea- surements of 0.98 (p<0.0001), 0.96 (p<0.0001) and 0.96 (p<0.0001),respectively.
Thecorrespondingvaluesforend-systolicMAD,MAAand MAP were 0.03±0.21 cm, -0.03±0.39 cm2 and 0.03±0.43 cm,with correlation coefficientsof 0.97 (p<0.0001),0.98 (p<0.0001)and0.98(p<0.0001),respectively(interobserver variability). The corresponding parameters for intraob- servervariabilityincludingtwomeasurementsbyobserver 1 were -0.02±0.21 cm, -0.01±0.34 cm2 and 0.03±0.53 cm, respectively, with correlation coefficients between theseindependentmeasurementsof0.98(p<0.0001),0.98 (p<0.0001)and0.97(p<0.0001),respectively.
Discussion
In the early stages of acromegaly, excess hGH and IGF-1 induce a hyperkinetic syndrome. Subsequentlyconcentric hypertrophy develops, togetherwith LVdiastolic dysfunc- tion and eventually impaired systolic function, ending in heart failure unless the excess hGH/IGF-1 is treated.3 Hypertension,arrhythmias,atherosclerosis,coronaryartery diseaseandheartvalvediseasearealsofrequentfindingsin acromegaly.3
Acromegaly has been found to be associated with an increasedprevalenceofregurgitantvalvularheartdisease, whichisdependentonthedurationofexposuretoincreased hGH concentrations.11 Aortic valve regurgitation (≥trace severity)waspresent in 30%of acromegalicpatients, and mitral regurgitation (≥moderate severity) was present in 5%ofindividualswithacromegaly.11 Theoverallprevalence of valve abnormalities is higherin both active and cured acromegalic patients. The persistence of valve disease in patients withcuredacromegaly islikelytocorrelate with thepersistenceofLVhypertrophy.12
Undernormal,healthyconditions,thecontractilefunc- tionofthemyocardiuminthebasalregionsoftheleftatrium
and ventricle adjacent to the mitral annulus results in a sphincter-likemotionoftheannulus,whichisaninnervated fibrousring. Thissphincter-likenarrowingfollowsthecar- diaccycle.13Thecircumferentialfibersinthebasalsegment oftheleftatriumarepositionedsothattheircontraction createsacentripetalforceontheinnersegmentoftheadja- centfibrousMAring,leadingtoaninwardmotionduringlate diastole.The superficialobliquefibersof theLVinletgen- erateatorsionalforce ontheoutersegmentofthemitral annulus,causing it to move inwards in systole.13 Myocar- dialcontraction ofthe leftatriumandventriclefollowing thecardiaccycleandoccurringattheappropriatetimeare requiredforpropercontractionofthemitralannulus.13,14
In the present study, MA dilation with preserved func- tion was demonstrated in acromegalic patients with no significantmitralregurgitationandwithnorelationship to thedisease’sactivity.In3D-STEstudiesfordeeperinsights intoacromegaly-associatedabnormalities,impairedLVrota- tionalmechanics has been found, with reducedapical LV rotationand LVtwist and 20% incidenceof absence of LV twist (LV rigid body rotation) in acromegalic patients.15 Moreover, increased LV radial strains have been demon- strated,togetherwithchangesinLAfunctionalparameters, suggestingcompensatoryincreasesinLVandLAcontractil- itytomaintainLVpumpingfunction.16---18Theseresultscould explainboththeMAdilationanditsnormalfunction,help- ing to elucidate these particular features of acromegalic cardiomyopathy.
These results highlight the need for reliable non- invasiveassessment of MA dimensionsin clinical practice.
AlthoughtrueMAdiameterisunderestimatedbyroutine2D echocardiography,6transthoracicreal-time 3Dechocardio- graphy(RT3DE)hadbeenvalidatedbymagneticresonance imaging for the assessment of MA dimensions and offers superior accuracy to 2D echocardiography, but its main limitationisthatitmeasuresthe2D-projectedannulus,not itsreal3D-shape.6---8TransesophagealRT3DE(RT-3DE)using specialsoftwareisabletocreateavirtual3Dmodelofthe mitralvalve andits annulus, but due toits semi-invasive nature its usefulness is limited.19 Although 3D-STE is
optimal for simultaneous assessment of strain, rotational andvolumetricparametersoftheheartchambersusingthe sameacquired3Dechocardiographicdataset,transthoracic 3D-STE has a similarability to transesophageal RT-3DE to visualizetheannulus.Itiseasytouse,thelearningcurveis short,thereisnoradiation,itscostisrelativelylow,andit canbeusedinasymptomaticnon-cardiacpatientssuchas individualswithacromegaly.20
Studylimitations
Inourpatients,acromegaliccardiomyopathywaspresentin bothearlyandlaterstages,whichcouldaffecttheresults.
3D-STEis anew methodologywithlimitedspatial (dueto the limited number of piezoelectriccrystals) and tempo- ralresolution(mean25±5framespersecond),whichcould affectimageresolutionandquality.Withthepresented3D- STE-derivedMAanalysis,the3Dsaddleshapeoftheannulus cannot be analyzed, only its 2D projection, which could theoretically affectthe measurements. The present study didnotaimtoassessandcompare3D-STE-derivedLV,left or right atrial volumetric and strain parameters between acromegalicpatientsandmatchedcontrols.
Conclusions
MAdilationwasseeninacromegalyregardlessofitsactivity.
Acromegaly is not associated with MA functional impair- ment.
Conflicts of interest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.MelmedS.Acromegaly.NEnglJMed.1990;322:966---77.
2.SchöflC,Petroff D,TönjesA, etal.Incidence ofmyocardial infarctionandstrokeinacromegalypatients:resultsfromthe GermanAcromegalyRegistry.Pituitary.2017;20:635---42.
3.VitaleG,PivonelloR,LombardiG,etal.Cardiacabnormalities inacromegaly.Pathophysiologyand implicationsfor manage- ment.TreatEndocrinol.2004;3:309---18.
4.Lombardi G, Galdiero M, Auriemma RS, et al. Acromegaly and the cardiovascular system. Neuroendocrinology.
2006;83:211---7.
5.SilbigerJJ. Anatomymechanics, and pathophysiology of the mitralannulus.AmHeartJ.2012;164:163---76.
6.Anwar AM, Soliman OI, ten Cate FJ, et al. True mitral annulus diameter is underestimated by two-dimensional
echocardiographyasevidencedbyreal-timethree-dimensional echocardiographyandmagneticresonanceimaging.IntJCar- diovascImaging.2007;23:541---7.
7.Anwar AM,SolimanOI,NemesA, etal.Assessmentofmitral annulussizeandfunctionbyreal-time3-dimensionalechocar- diography in cardiomyopathy: comparison with magnetic resonanceimaging.JAmSocEchocardiogr.2007;20:941---8.
8.Nemes A, AnwarAM, CaliskanK, etal. Non-compactioncar- diomyopathyisassociatedwithmitralannulusenlargementand functionalimpairment:areal-timethree-dimensionalechocar- diographicstudy.JHeartValveDis.2008;17:31---5.
9.LangRM,BadanoLP,Mor-AviV,etal.Recommendationsforcar- diacchamberquantificationbyechocardiographyinadults:an updatefromtheAmericanSocietyofEchocardiographyandthe European Associationof Cardiovascular Imaging.EurHeart J CardiovascImaging.2015;16:233---70.
10.Nemes A, Kalapos A, Domsik P, et al. Three-dimensional speckle-tracking echocardiography --- a further step in non-invasive three-dimensional cardiac imaging. Orv Hetil.
2012;153:1570---7.
11.PereiraAM,vanThielSW,LindnerJR,etal.Increasedpreva- lenceofregurgitantvalvularheartdiseaseinacromegaly.JClin EndocrinolMetab.2004;89:71---5.
12.ColaoA,SpinelliL,MarzulloP,etal.Highprevalenceofcardiac valvediseaseinacromegaly:anobservational,analytical,case- controlstudy.JClinEndocrinolMetab.2003;88:3196---201.
13.SilbigerJJ,BazazR.Theanatomicsubstrateofmitralannular contraction.IntJCardiol.2020;306:158---61.
14.MihailaS,MuraruD,MiglioranzaMH,etal.Normalmitralannu- lusdynamicsanditsrelationshipswithleftventricularandleft atrialfunction.IntJCardiovascImaging.2015;31:279---90.
15.KormányosÁ,DomsikP,KalaposA,etal.Leftventriculartwist isimpairedinacromegaly:insightsfromthethree-dimensional speckletrackingechocardiographicMAGYAR-PathStudy.JClin Ultrasound.2018;46:122---8.
16.KormányosÁ,DomsikP,KalaposA,etal.Activeacromegalyis associatedwithenhancedleftventricularcontractility---Results fromthethree-dimensionalspeckle-trackingechocardiographic MAGYAR-PathStudy.RevPortCardiol.2020;39:189---96.
17.Edvardsen T. How to interpret assessment of left ventric- ular function by strain in acromegaly? Rev Port Cardiol.
2020;39:197---8.
18.Kormányos Á, Domsik P,KalaposA, et al. Three-dimensional speckle tracking echocardiography-derived left atrial defor- mationanalysisinacromegaly(ResultsfromtheMAGYAR-Path Study).Echocardiography.2018;35:975---84.
19.SköldborgV,MadsenPL,DalsgaardM,etal.Quantificationof mitralvalveregurgitationby2Dand3Dechocardiographycom- paredwithcardiacmagneticresonanceasystematicreviewand meta-analysis.IntJCardiovascImaging.2020;36:279---89.
20.Nemes A, Kovács Z,Kormányos Á, et al. Themitral annulus in lipedema: Insights from the three-dimensional speckle- trackingechocardiographicMAGYAR-PathStudy.Echocardiogra- phy.2019;36:1482---91.