73 Table 10: Association between work-family conflict and lack of social (ie parental, spouse, peer and organizational) support among. 77 Table 12: Gender differences in the prevalence of self-reported psychological and somatic morbidity among doctors.
Preamble
The increasing importance of the work-home interface
- The traditional nature of the Hungarian society: gender role
- Population ageing
- Increasing participation of women in the workforce
- Increasing demands at work to improve productivity
- Inadequate organizational response
However, women in Hungary are unlikely to abandon their non-working roles (eg mother, wife, caregiver, etc.) in the foreseeable future due to the traditional nature of society and its continued reinforcement through socialization. The current, broadly similar employment rate for women in the EU and Hungary is the result of two different processes in the labor force.
Conflict at the work-home interface: work-family conflict
An inappropriate organizational response, therefore, may have the potential to exacerbate the conflict at the work-home interface as perceived by many women and especially female physicians. Data published nearly thirty years ago shows that 58% of female physicians reported conflict between work and family (Nadelson, Notman, & Lowenstein, 1979).
Work-family conflict and stress: the theory of roles and the stress
Antecedents to stress
- Work stressors
- Home stressors
- Socio-demographic stressors
- Work-family conflict as a stressor
This approach is particularly important in the study of work-family conflict, as it emphasizes the interdependence and multi-directionality of the various contributors to stress in an individual's life. Therefore, it has been suggested that work-family conflict should be considered a separate construct within the stress response (Frone, et al., 1992a).

Potential outcomes of the stress response
- Organizational and societal outcomes of the stress response
- Individual outcomes of the stress response: adverse impact on
Other features of the immune system may be running unchecked, increasing the risk of developing or exacerbating autoimmune diseases (Quick et al., 1997; McEwen, 1998; Gareau, et al., 2008). Studies also suggest that chronic activation of stress hormones may alter the action and structure of neurons critical to memory formation and function (Quick et al., 1997; McEwen, 1998).
The well-being of physicians: associations with stress
Psychological morbidity including burnout
- Major symptoms of burnout
- The development of burnout
Most previous studies have concentrated on physicians' mental health and found high prevalence of significant psychological illnesses, including depression, suicidal ideation, substance abuse, stress, and stress-related illnesses among physicians (Shanafelt, et al., 2003). Although many doctors acknowledge the existence of these stresses, it is difficult to fully understand their effect on doctors' health.
The psycho-social characteristics of work-family conflict
Potential antecedents to work-family conflict experienced by
Research by Burke (1988) found that a lack of support in the non-work environment was associated with work-family conflict in a sample of police officers. In a study of nurses, Gottlieb, Kelloway, and Martin-Matthews (1996) identified a lack of social support as a predictor of work-family conflict.
Potential consequences of perceived work-family conflict among
A further aim of this research was therefore to examine the prevalence and psychosocial characteristics of parental, marital, peer and organizational support and their relationships to work-family conflict. Therefore, the final aim of this research was to evaluate the prevalence of organizational and individual distress outcomes (i.e. job satisfaction, somatic and psychological morbidity, especially burnout) and to find associations between these distress outcomes and perceived work-family conflict among female physicians in the Hungarian context.
The conceptual framework and hypotheses of this research
Despite the high likelihood of work-family conflict as a source of distress among female physicians, its association with organizational and individual distress outcomes such as job satisfaction, burnout, other psychiatric/psychological illnesses, and somatic problems are major determinants of physician health. creature, are not fully explored. Conflict between work and family is associated with psychological morbidity, especially burnout, somatic problems, as well as job dissatisfaction among female doctors.
Design
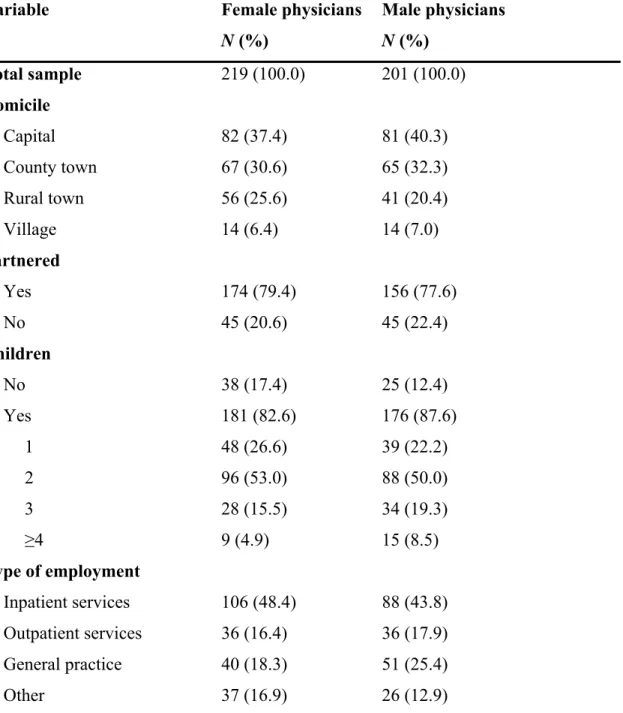
Sample
The results of the goodness-of-fit tests confirmed that the distribution of our sample was comparable to the distribution of the normative population in terms of gender, age, and residency and the two main specialties (i.e., internists and paediatrics), suggesting that our results could be generalizable doctors in Hungary (Table 3). According to this test, the error with 90%, 95%, and 99% confidence levels was 4%, 4.8%, and 6.2%, respectively, suggesting that our results may adequately represent the normative population.
Measuring instruments
- Work-family conflict
- Job demands, job control, job strain, and support in the
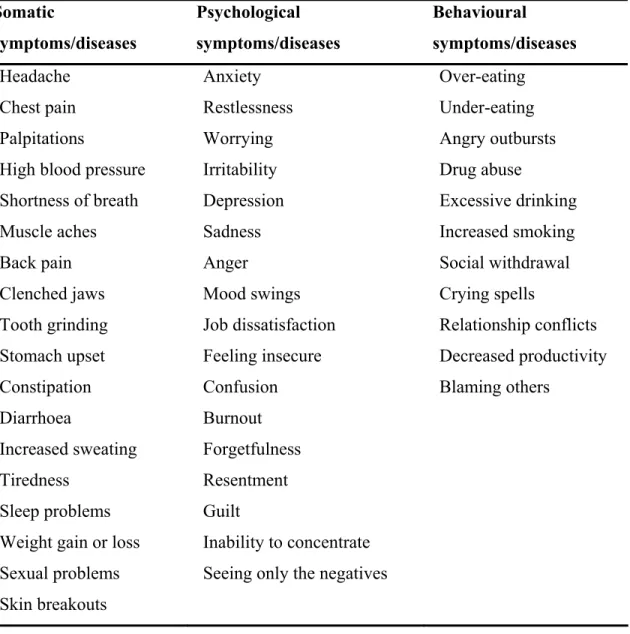
- Measures of psychological and somatic morbidity
- Perceived anxiety
- Physician burnout
- Job satisfaction
The reliability coefficients (Cronbach's alpha) for the emotional exhaustion, depersonalization and personal achievement scales for our total sample were, respectively. 0.80. Job satisfaction was defined as a match between expectations and the perceived reality of the job (Bacharach, Bamberger & Conley, 1991) and was assessed using a scale adapted from Scarpello and Campbell (1983) and Wanous, Reichers and Hudy (1997).
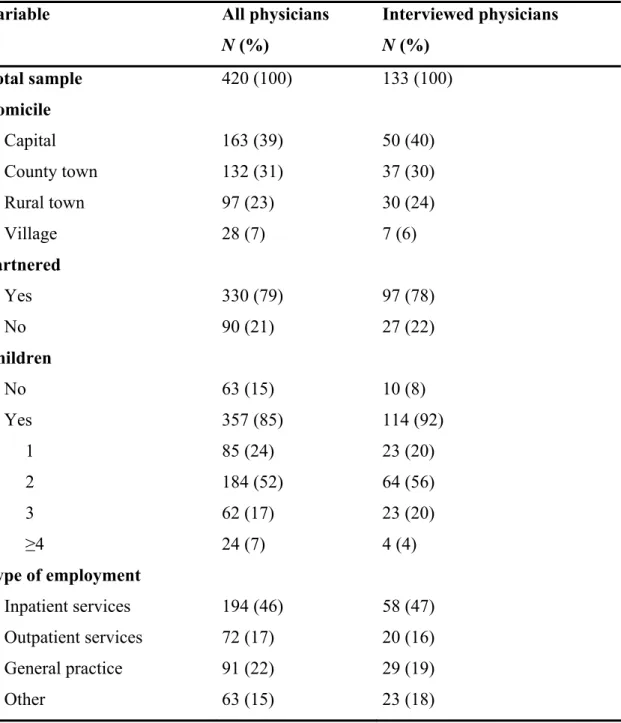
Interviews
After owner approval, if applicable, the instruments were translated from English into Hungarian and validated through back translation to ensure that both versions were equivalent. The tools were then provided to a small test group of female and male physicians (N=16), who appeared to interpret the questions related to the variables as we intended.
Data analyses
- Analyses to explore associations between work-family conflict and
- Regression analyses to identify potential antecedents to work-
- Analyses of gender differences in self-reported psychological and
- Regression analyses to identify stressors associated with
- Analyses to assess the level of job satisfaction and its associations
- Regression analyses to identify stressors associated with job
- Content analysis of interview data
Descriptive statistics were performed to assess the mean level of job satisfaction among female and male physicians, as well as in the entire sample. Differences in the level of job satisfaction between female and male physicians were investigated by independent samples t-tests. To explore the links between job satisfaction and work-family conflict, differences in the level of perceived work-family conflict between female and male physicians, as well as in the entire sample among those who reported a high degree of job satisfaction (a score of 4 or 5 on the job satisfaction scale) and those who did not (a score of 1, 2 and 3 on the job satisfaction scale) were assessed with independent samples t-tests.
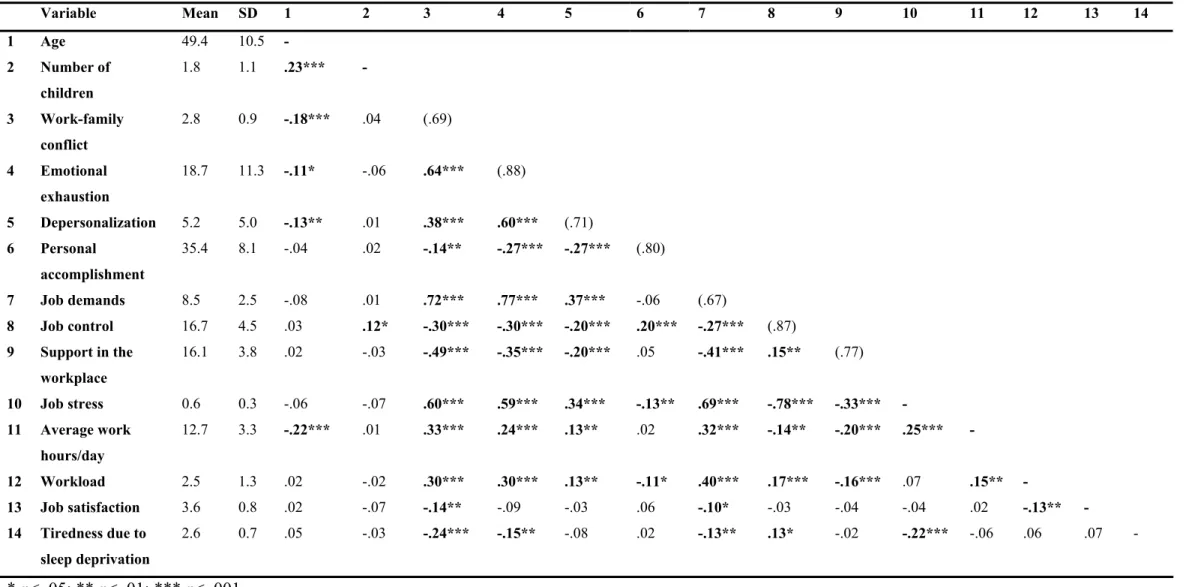
Intercorrelations among study variables
Fatigue due to lack of sleep does not appear to correlate with emotional exhaustion among male physicians (Table 6). Among male physicians and in the entire sample, depersonalization correlated well with all work-related variables except job satisfaction (Table 6 and Table 7). Among male physicians, job satisfaction showed only a significant inverse correlation with emotional exhaustion (r = -.14; p <.05) (Table 6).
High level and prevalence of work-family conflict among female
Gender disparity in the direction and type of work-family
Female physicians reported significantly more strain-based work-family conflict, while male physicians experienced significantly more time-based work-family conflict. The prevalence of behaviorally based work-family conflict was relatively low among physicians (about 10%). I ran home after work to take care of my family, including my husband, and sometimes during work to check on my kids.

Gender differences in perceived social (i.e., parental, spousal, peer,
One theme was the access or availability of same-sex professional role models or mentors during career choice, medical training, or professional life, and another was the lack of gender-based discrimination, which physicians operationalized as providing equal opportunities in the workplace to men and women through non-discriminatory behavior , actions, procedures or interactions with peers or the lack of a hostile or intimidating environment. Significantly more physicians than physicians reported that lack or lack of access to same-sex professional role models may have contributed to their level of perceived distress (79% vs. 43%) (Table 9). A lack of organizational support, including family-friendly policies such as crèches and kindergartens, flexible working hours, counseling or part-time work, was identified by about half of the female doctors (Table 9), but only female doctors mentioned the links between the lack of organizational support and distress.
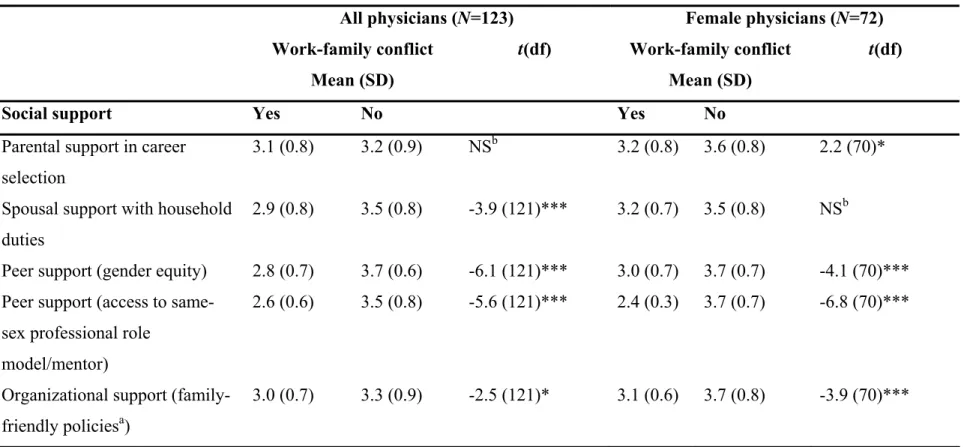
Work-family conflict is associated with lack of social (i.e., parental,
10 Physicians who experienced a lack of partner, peer (i.e., access to same-sex role model/mentor or gender equality) or organizational (i.e., family-friendly policies) support reported significantly higher levels of work-family conflict compared to those who did experience social support . As hypothesized, female physicians (N=72) who lacked support from parents, peers, or organizations experienced significantly more work-family conflict compared to those who lacked social support. The lack of instrumental support of marriage among female physicians was not associated with a higher level of work-life conflict.
Stressors associated with work-family conflict: lack of support in
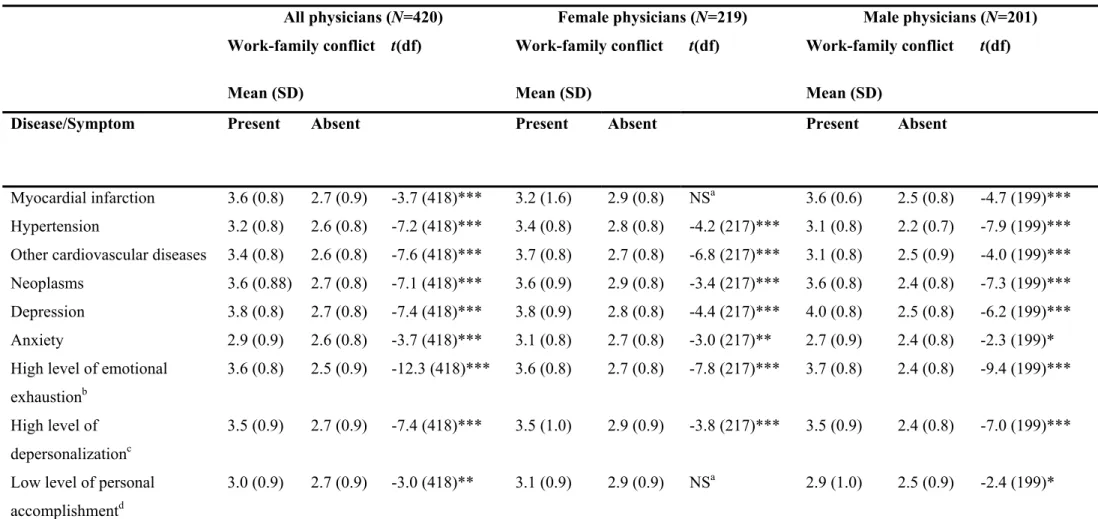
High prevalence of somatic and psychological morbidity among
Associations between work-family conflict and both somatic and psychological morbidity were examined with a series of independent sample t-tests. Among female physicians, the prevalence of myocardial infarction, low level of personal competence, and neurological diseases did not seem to correlate significantly with a higher level of work-life conflict. However, strong associations of work-life conflict were observed with all other previous conflicts. mentioned diseases and in addition with gynecological diseases. Work-family conflict showed significant associations with all previously mentioned diseases except neurological diseases among male physicians.

Stressors associated with somatic and psychological morbidity
All doctors (N=420) Female doctors (N=219) Male doctors (N=201) Work-family conflict Work-family conflict Work-family conflict.
Stressors associated with burnout: work-family conflict as a
Significantly lower prevalence of job satisfaction and higher
Work-family conflict is associated with job satisfaction among
Stressors associated with job satisfaction: work-family conflict as a
These predictors explained about 4%, 7% and 2% of the variance in job satisfaction among the total population, female and male doctors, respectively (Table 18). This study investigated the manifestation, direction, and type of self-reported work-family conflict as a significant source of stress among a rarely studied group of physicians in a unique cultural setting with a presumed central role of the family as an institution. In addition, the study examined the manifestation of physician well-being by assessing the prevalence of job satisfaction and psychological and somatic morbidity, including self-reported burnout, and explored their association with work-family conflict experienced by physicians and physicians.

Manifestation of work-family conflict among physicians
Our results also show important gender-specific differences in the direction and type of work-family interference. There are very few studies to date that have examined gender differences in work-family conflict and its potential psychosocial characteristics (Frone, et al., 1992a). We also identified gender differences in the type of work-family conflict, showing that female physicians experienced strain-based work-family conflict significantly more frequently, while men mostly reported time-based work-family interference.
Potential antecedents to work-family conflict experienced by
The psychosocial characteristics of social support
- Lack of parental support and female professional role model or
- Lack of gender equity
- Lack of spousal support for women
- Lack of organizational support
A lack of interaction and support from female professional role models or mentors can therefore contribute to confirming the discrepancy between work and family. A large proportion of doctors felt that their organization was not supportive due to the limited provision of family-friendly policies that would enable a better integration of the professional and domestic spheres and consequently reduce the conflict between work and family. It is therefore necessary to implement mechanisms and policies to ease tensions and prevent the development of conflicts between work and family.
Potential consequences of work-family conflict experienced by
Poor psychological health among Hungarian physicians
- Manifestation of physician burnout
Our results regarding the prevalence of self-reported depression among physicians (about 8%) are comparable to these findings. Our results show that the self-reported prevalence of suicidal ideation (reported as other psychiatric/psychological illness) among physicians was about 2%. Furthermore, the prevalence of suicidal ideation among female physicians was as high as among male physicians (Győrffy, et al., 2005b).
Poor somatic health among Hungarian physicians
Conversely, our data shows that only about 3% of female doctors in Hungary worked part-time. Based on our findings on the high prevalence of somatic and psychological morbidity among female and male physicians and the lack of consistent gender differences in their prevalence, we argue that it cannot be concluded that the health status of female physicians is generally worse than that of female physicians. male doctors. Another possible explanation for the excessive mortality among female doctors could be the gender differences in healthcare behavior.
High prevalence of job dissatisfaction among Hungarian
Our results seem to confirm this finding, as the degree of job satisfaction among female and male physicians was similar. This is an interesting finding, as female physicians in our study reported higher levels of work-life conflict, a form of tension that has been associated with lower levels of job satisfaction (see below). Personal performance among female physicians and a lack of emotional exhaustion among male physicians emerged as significant predictors of job satisfaction.
Associations between poor psychological as well as somatic health
Associations between burnout and work-family conflict
The relationship between work-family conflict and burnout experienced by physicians has been examined in a number of studies. 1999) identified work-family interference as a mediator between job characteristics and burnout (that is, emotional exhaustion and depersonalization). Our results indicate that physician burnout, and emotional exhaustion in particular, is best predicted by work-family conflict, along with other job stressors, such as higher job demands and a lack of job control.

Limitations of this research
The importance of different practice settings (e.g. work in educational or research institutions) in predicting depersonalization and lower personal performance is an interesting finding in our study and deserves further research. identified as a dependent variable. 1996) found that the higher the work-to-family conflict, the lower the emotional and instrumental support from the family. Bidirectional relationships between support and the different forms of work-family conflict require further research. In addition, the relationship between work-family conflict and somatic as well as psychological morbidity including burnout may have been influenced by negative affectivity defined by Watson and Clark (1984) as a stable tendency to express emotions across time and situations.
Strengths of this research
However, recent research suggests that negative affectivity does not unduly distort relationships between self-report measures of stressors and strain (e.g., Schonfield, 1996; Dollard & Winefield, 1998; de Jonge, Dormann, Janssen, Dollard, Landeweerd, & Nijhuis, 2001). This research also provides some justification for advocating urgent preventive measures to reduce work-family conflict, which may subsequently improve the well-being of women in medicine. Our research also contributes to current efforts to establish national norms for the MBI in cross-cultural burnout research.
Future directions for empirical research on work-family conflict116
The role enhancement theory
The spillover theory
The conservation of resources theory
The self-discrepancy theory
The social identity theory
The social exchange theory
Level, focus, scope, and methodology of future research
This research examined the level, prevalence, psychosocial characteristics and antecedents of work-family conflict (WFC), as well as its relationships with organizational (job satisfaction) and individual (somatic as well as psychological morbidity including burnout) stress outcomes using quantitative and qualitative stress outcomes. techniques among doctors (N=420) in Hungary. Relationship of work-family conflict to health outcomes: A four-year longitudinal study of working parents. High prevalence of work-family conflict among female physicians: lack of social support as a potential antecedent.
High prevalence of work-family conflict among women doctors in Hungary: sources and adverse health outcomes. High prevalence of work-family conflict among female physicians: lack of individual and organizational support as potential antecedents.